Chapter Headings
Introduction
The Diabetes Canada Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada (CPG) were last published in 2018 (1). New evidence has been published since the 2018 guidelines, prompting this update to our recommendations for Chapter 13, “Pharmacologic Glycemic Management of Type 2 Diabetes in Adults” (1).
What’s New in 2020
First, additional agents approved for use in Canada have been shown to have cardiovascular (CV) benefits in patients with type 2 diabetes. Second, some of these CV benefits have now been demonstrated in people with CV risk factors but without established atherosclerotic cardiovascular disease (ASCVD). Third, there is more evidence showing that sodium-glucose cotransporter-2 inhibitors (SGLT2i) reduce the risk of hospitalization for heart failure (HHF) and the progression of chronic kidney disease (CKD). Finally, additional studies of comparative effectiveness of antihyperglycemic agents provide stronger evidence that glucagon-like peptide-1 receptor agonists (GLP1-RA) and SGLT2i are associated with greater weight loss compared to other agents.
We have, therefore, added new recommendations or updated existing recommendations based on rigorous and careful review of the evidence regarding the efficacy on clinically important outcomes and adverse effects of available medications. Minor changes to wording have also been made to some recommendations for enhanced clarity. The revised recommendations, treatment algorithm (Figures 1, 2A, 2B, 3), list of available agents (Table 1) and summary of CV outcome trials (CVOT) (Table 2), with a rationale and summary of the supporting trials, are presented here to assist practitioners as they approach antihyperglycemic therapy for people with type 2 diabetes.
The requirement for health-care providers to consider multiple factors when selecting antihyperglycemic medications is unchanged. These include degree of hyperglycemia; efficacy of agents for reducing diabetes complications and blood glucose levels; medication effects on the risk of hypoglycemia, body weight, concomitant medical conditions, and other side effects; ability to adhere to regimen; broader health and social needs; affordability of medications; and patient values and preferences.
Further revisions to the text of the chapter and related appendices will be published on the Diabetes Canada guidelines website (guidelines.diabetes.ca).
Methods
The overarching goals and methodologic principles for the Diabetes Canada CPG are unchanged from 2018 (2,3). Leveraging the search methods and PICO questions used for the 2018 CPG, a systematic search of the literature for relevant articles published from October 2017 to October 2019 was performed by health science librarians from the McMaster Evidence Review and Synthesis Team (MERST). The search was limited to studies conducted in humans and excluded phase 2 and phase 3 studies of antihyperglycemic agents where there was no active comparator. The MERST team reviewed all relevant citations at title and abstract, and full-text levels. Relevant citations that could potentially lead to new or modified recommendations were abstracted and critically appraised by a methodologist from MERST. The full-text citations and critical appraisal reports were provided to the expert working group who also critically appraised the citations, graded the evidence and drafted the revised recommendations. In general, the grading of the whole trial was applied to all recommendations supported by the trial, even if this represented a subset of the study population, unless there was evidence for heterogeneity between subgroups.
The composition of the expert working group and the Steering Committee, and the approach to disclosure and management of conflicts of interest, were aligned with recommendations of the CPG Interim Committee. These recommendations have been incorporated in a draft process manual which (when finalized) will be published and updated on the Diabetes Canada website. The working group members either had no direct financial links to industry partners or were compliant with institutional policies regarding interactions with industry. The Steering Committee includes women and men, different health-care professions, end-users and persons with lived experience of diabetes.
Two members of the Steering Committee conducted an independent assessment of the grading. A small group of clinicians with expertise in dissemination and implementation evaluated the draft recommendations for clinical applicability and helped develop the figures. The whole process was overseen by the CPG Chair and VP, Science and Policy, Diabetes Canada. The finalized recommendations were unanimously approved by the Steering Committee.
Figure 1
At diagnosis of type 2 diabetes.
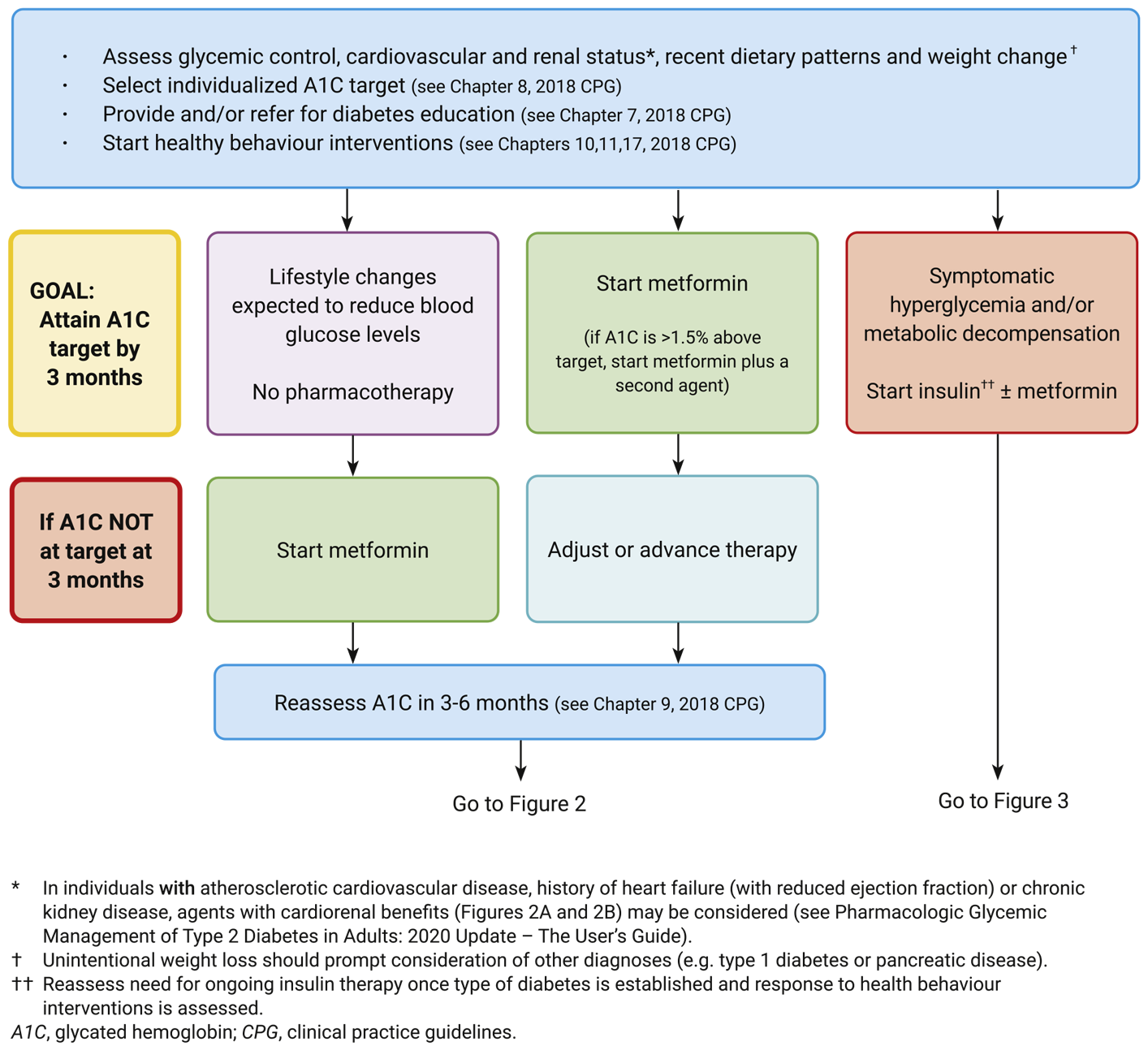
Figure 2A
Reviewing, adjusting or advancing therapy in type 2 diabetes.
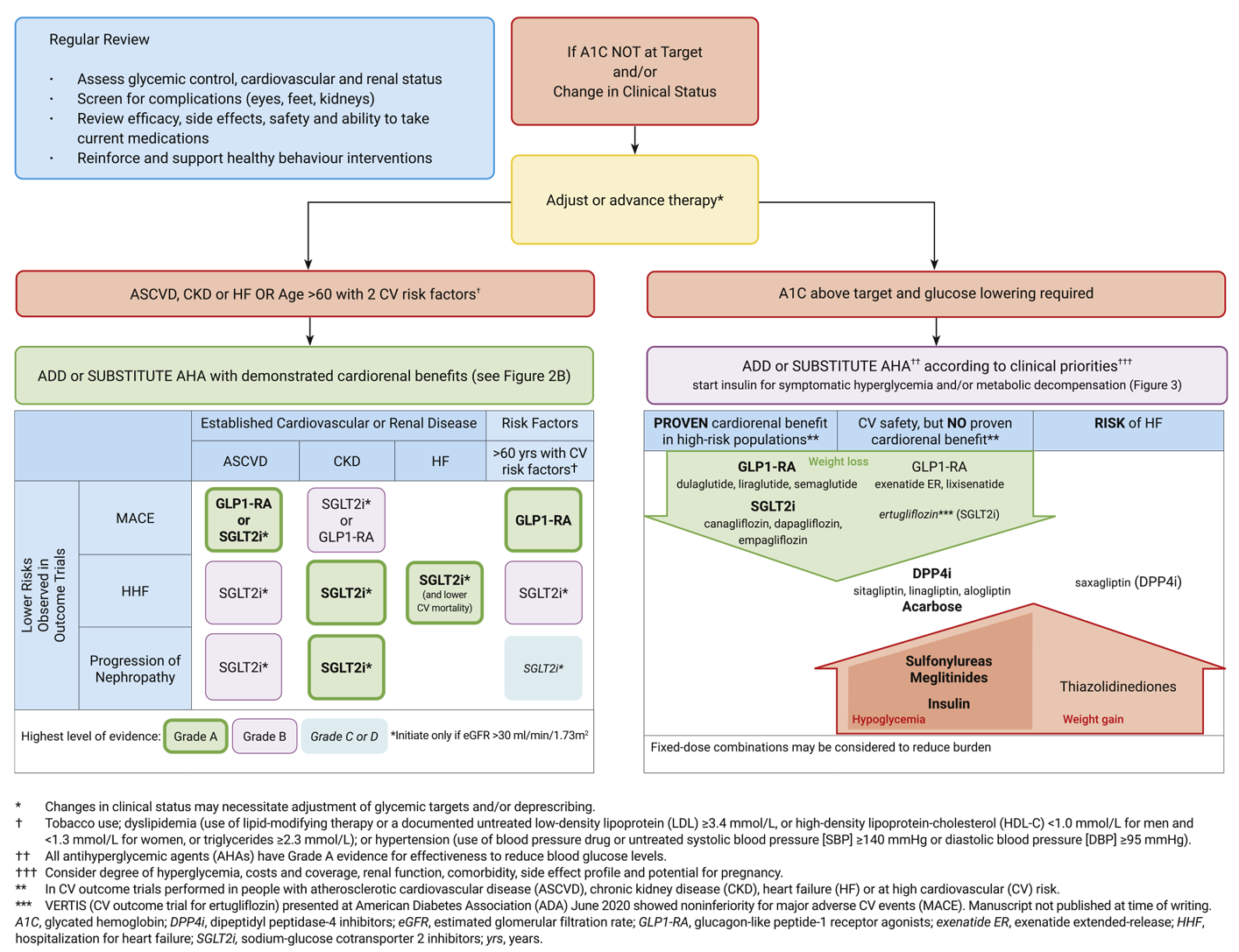
Figure 2B
Reviewing, adjusting or advancing therapy in type 2 diabetes.
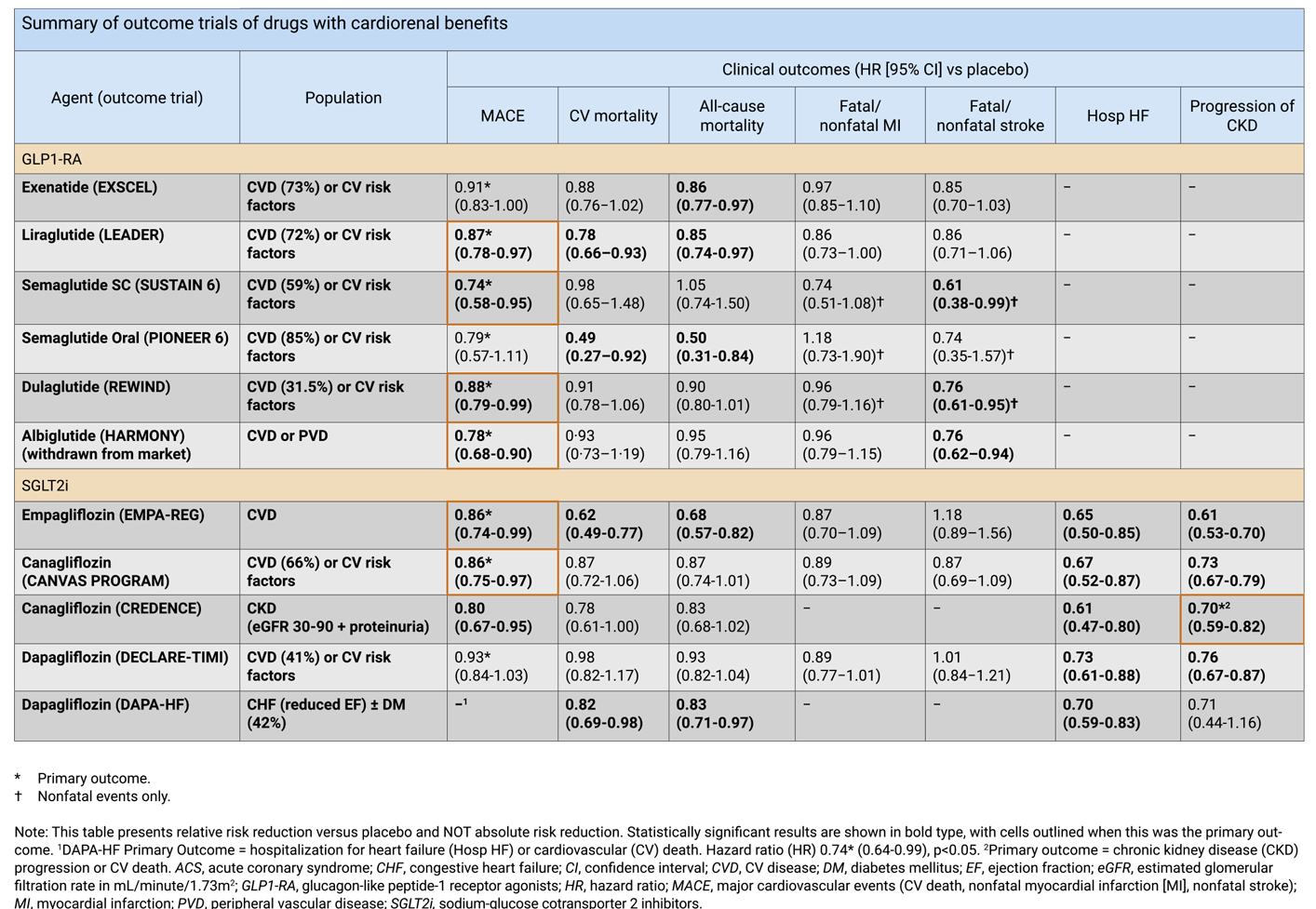
Figure 3
Starting or advancing insulin in type 2 diabetes.
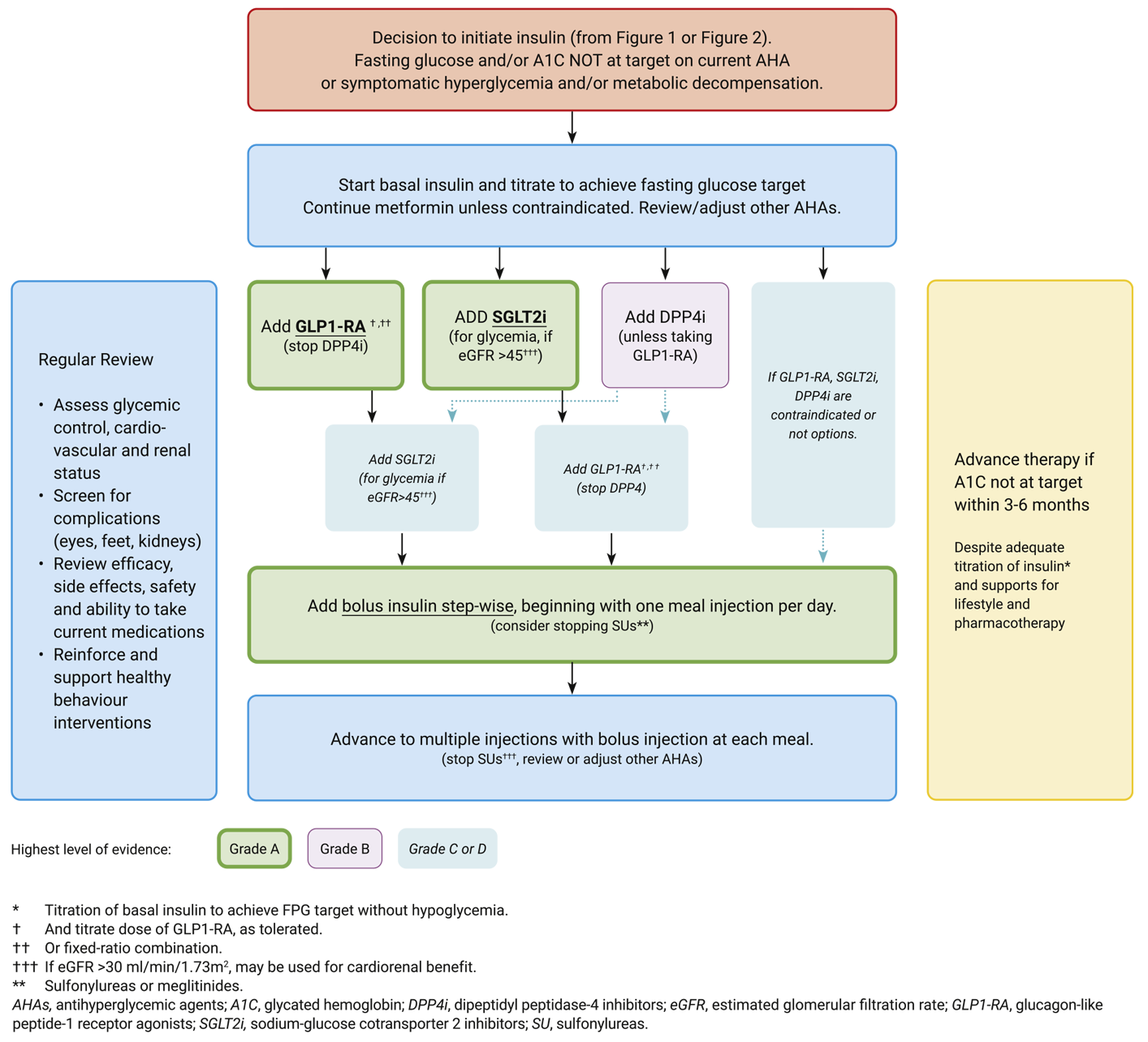
Table 1
Antihyperglycemic agents for use in type 2 diabetes.
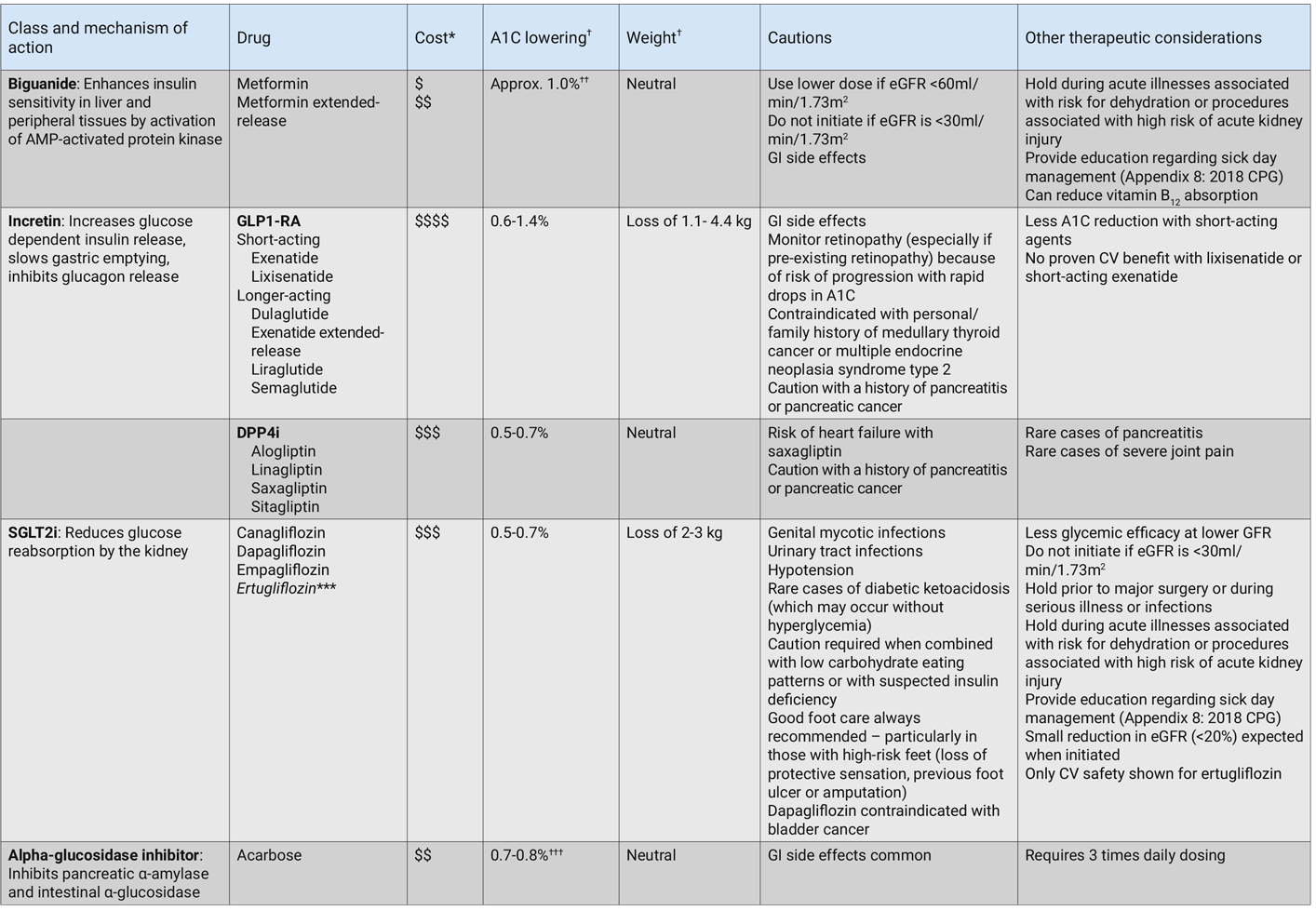
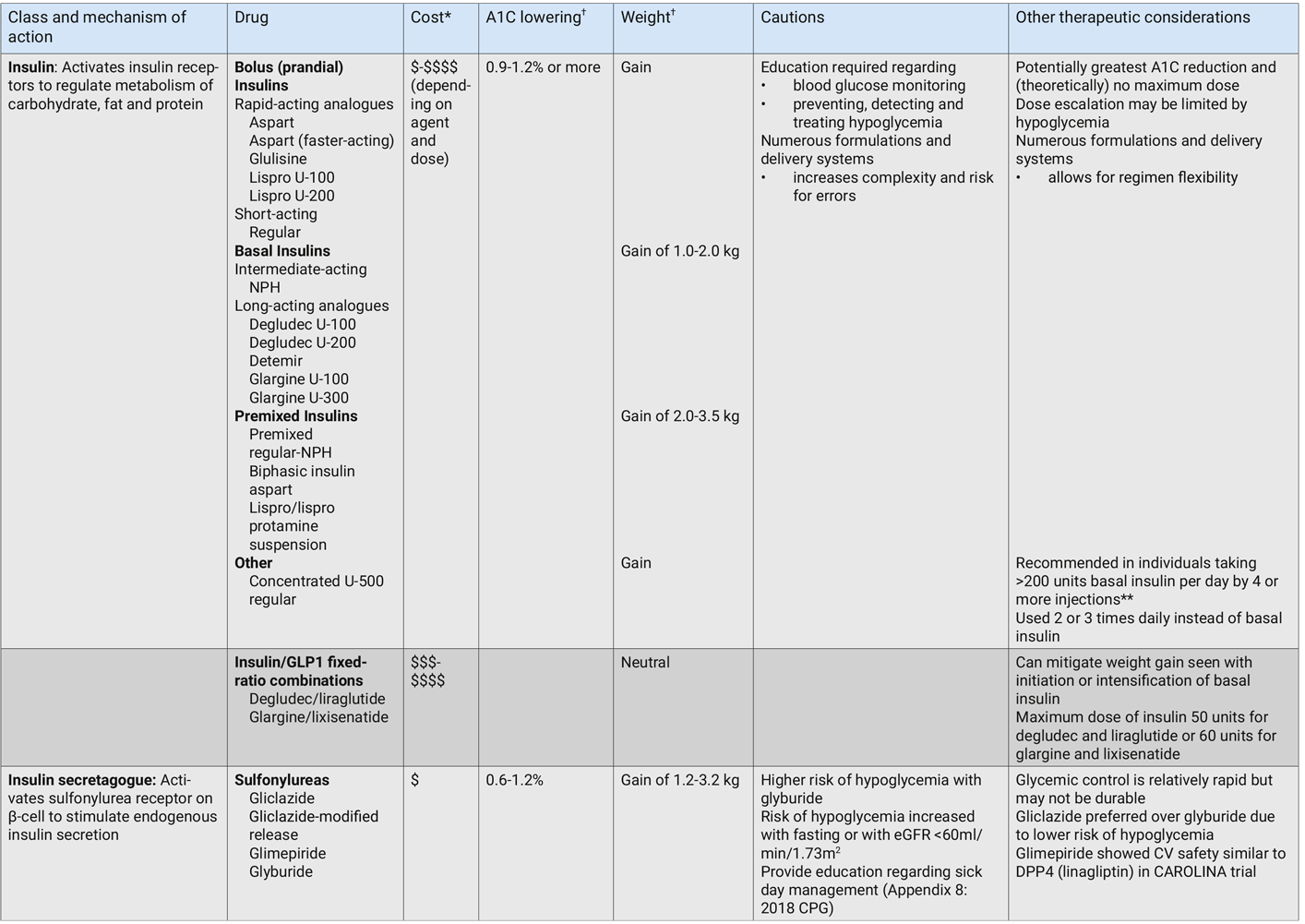
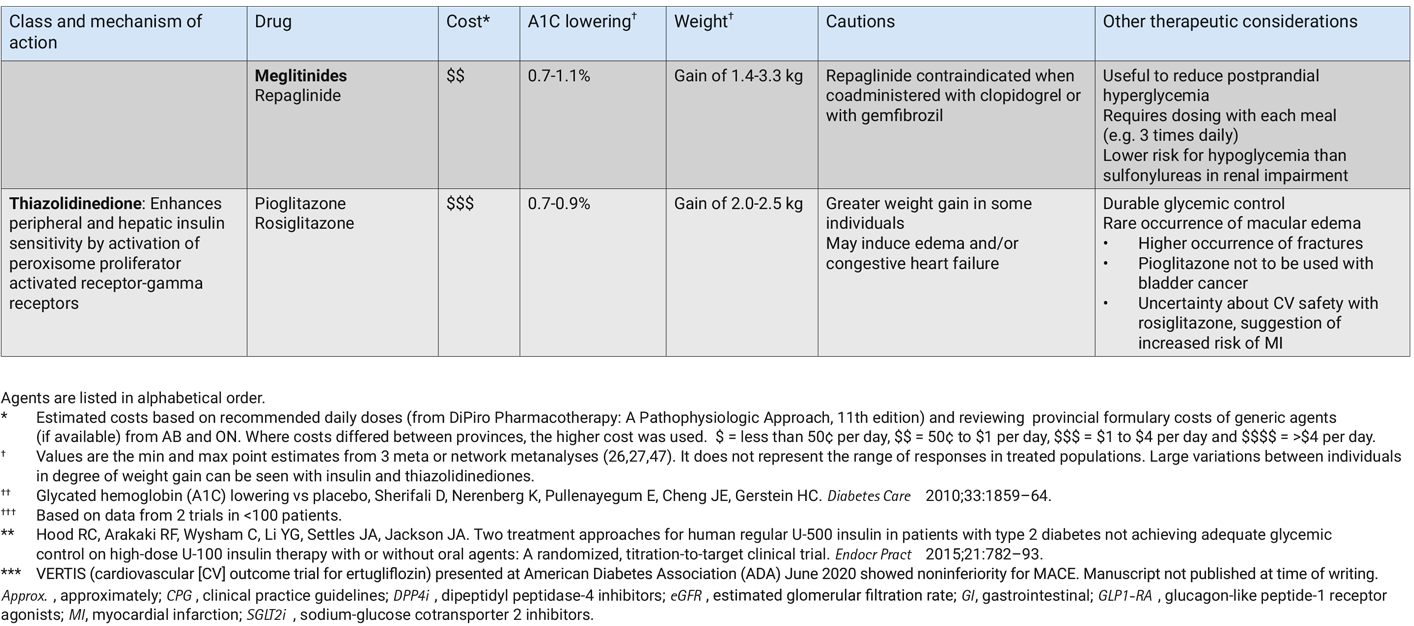
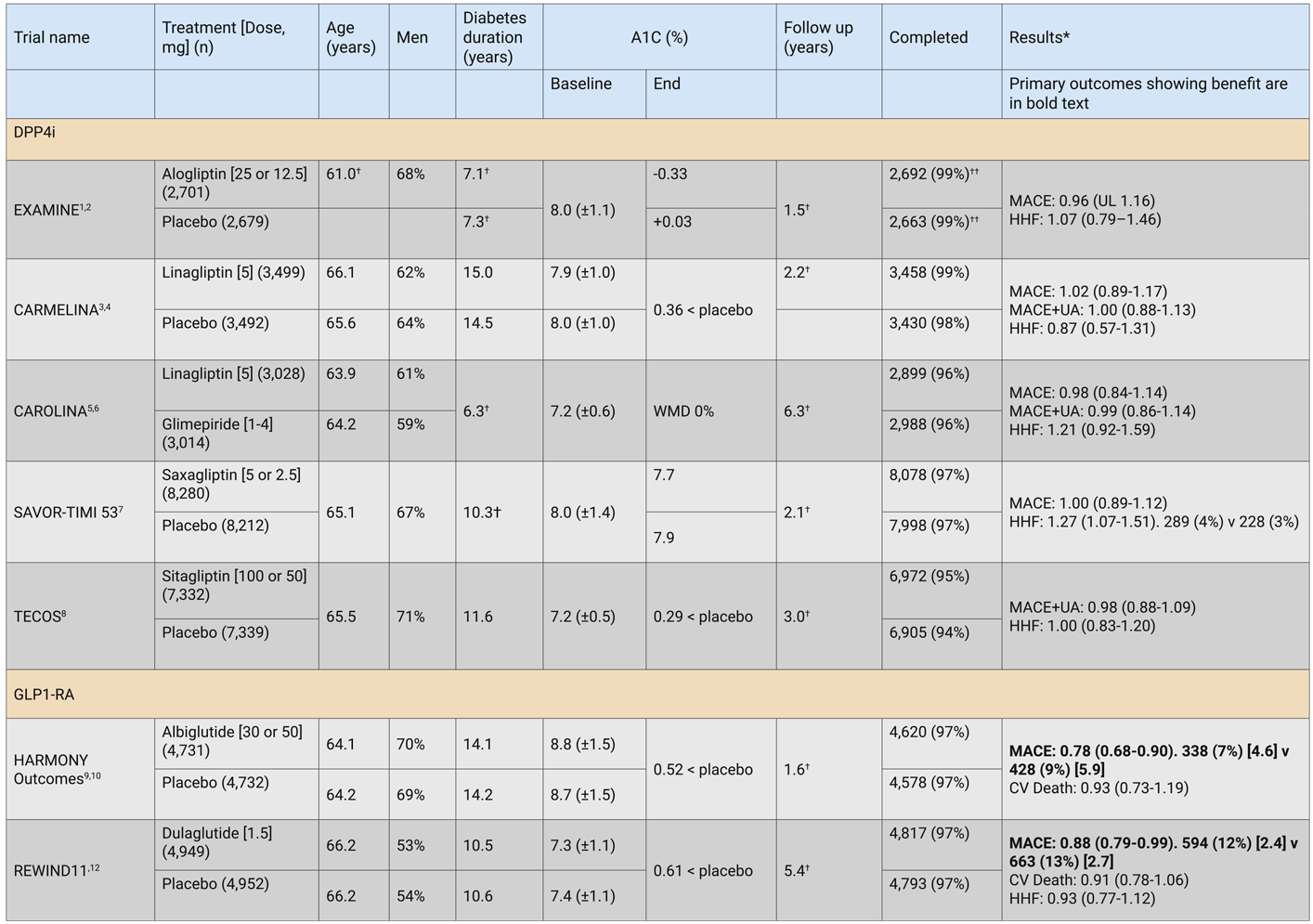
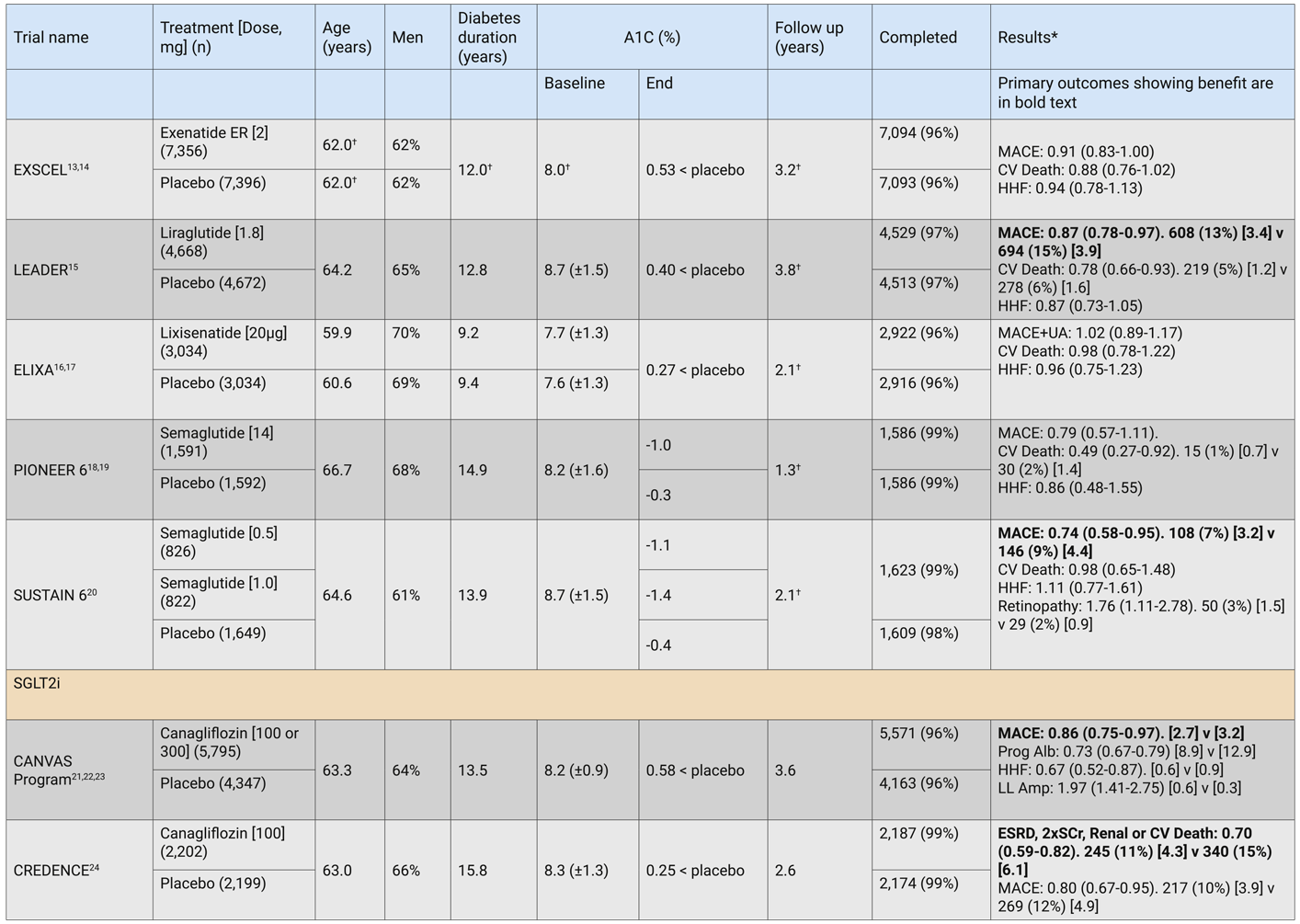
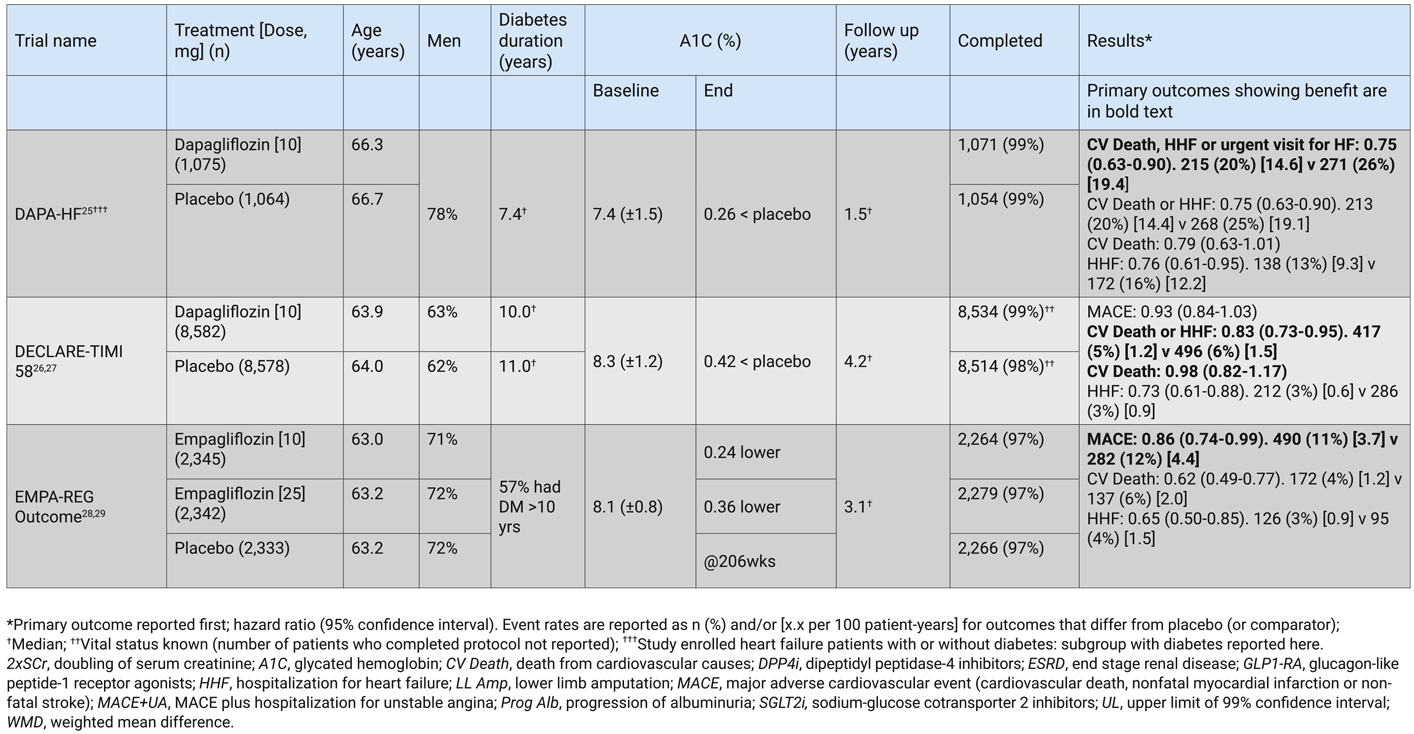
Table 2
Major clinical outcome trial characteristics for antihyperglycemic agents since US Food and Drug Administration guidance 2009.
| Table 3 Cardiovascular risk factors. |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| BP, blood pressure; HDL-C, high-density lipoprotein-cholesterol; LDL, low-density lipoprotein | ||||||||||
|
||||||||||
Rationale and Summary of Evidence Supporting Revision/New Recommendations
GLP1-RA
Secondary CV prevention in persons with ASCVD
Results of CVOT for 4 GLP1-RA, conducted largely in persons with pre-existing cardiovascular disease (CVD), were available at the time of publication of the 2018 guidelines. All GLP1-RA were noninferior to placebo with respect to major adverse CV events (MACE: nonfatal myocardial infarction [MI], stroke or CV death). Hazard rates for MACE were lower for liraglutide and subcutaneous semaglutide and extended release exenatide (nonsignificantly) compared to placebo. There was no suggestion of any CV benefit for lixisenatide.
Lixisenatide was compared to placebo in 6,068 patients with type 2 diabetes and a recent CV event over a median 2.1 years of follow up (MACE or hospitalization for unstable angina: 13.4% vs 13.2%; HR 1.02, 95% CI 0.89-1.17) (4). Extended-release exenatide was compared to placebo in 14,752 participants with type 2 diabetes (73% with pre-existing CVD) over a median 3.2 years of follow up (MACE 11.4% vs 12.2%; HR 0.91, 95% 0.83-1.00) (5). The first GLP1-RA to demonstrate significant CV benefit was liraglutide (6). The Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results (LEADER) trial evaluated CV outcomes in 9,340 participants with type 2 diabetes, of whom, 81% had established CVD or stage 3 or higher CKD and 72% had CVD only (6). Over a median follow up of 3.8 years, liraglutide was associated with a significantly lower incidence of MACE than placebo (13.0% vs 14.9%; HR 0.87, 95% CI 0.78–0.97), with significantly fewer CV deaths in patients treated with liraglutide compared to placebo (4.7% vs 6.0%; HR 0.78, 95% CI 0.66-0.93).
Since the 2018 guidelines were published, subcutaneous semaglutide became available in Canada and CVOT have been published for oral semaglutide, dulaglutide and albiglutide. Trials for those agents are described below (see also Table 2).
Subcutaneous semaglutide was compared to placebo in the phase 3a Trial to Evaluate Cardiovascular and Other Long-term Outcomes with Semaglutide in Subjects with Type 2 Diabetes (SUSTAIN-6) (7). Similar to the LEADER trial of liraglutide (6), patients were eligible if they had type 2 diabetes and an A1C of 7% or greater; and were age ≥50 years with established CVD or stage 3 or higher CKD or age ≥60 years with at least 1 CV risk factor (microalbuminuria or proteinuria, hypertension and left ventricular hypertrophy, left ventricular systolic or diastolic dysfunction, or an ankle–brachial index of less than 0.9). SUSTAIN-6 enrolled 3,297 participants with a mean duration of type 2 diabetes of 13.9 years and mean A1C of 8.7% (7), and they were randomized to subcutaneous semaglutide 0.5 mg or 1.0 mg weekly or placebo. At baseline, 98% were on antihyperglycemic therapy, 83% had established CVD or stage 3 or higher CKD, and 59% had CVD only. After a median follow up of 2.1 years, the primary composite outcome of MACE occurred in 6.6% of participants treated with semaglutide and 8.9% of participants treated with placebo (HR 0.74, 95% CI 0.58–0.95), fulfilling statistical criteria for noninferiority (p<0.001); a posthoc test for superiority was also significant (p=0.02). While the main findings from this trial were similar to those for liraglutide from the LEADER trial (6), as the hypothesis for CV benefit superiority was not prespecified, the evidence for CV benefit of subcutaneous semaglutide was graded lower than for liraglutide.
Oral semaglutide, the first orally available GLP1-RA, was evaluated in the phase 3a Oral Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes (PIONEER 6) trial (8). This study compared once-daily oral semaglutide to placebo in participants at high CV risk defined as age ≥50 years with established CVD or CKD, or age ≥60 years with CV risk factors only. PIONEER 6 enrolled 3,183 participants with a mean age of 66.7 years, mean A1C of 8.2% and mean 14.9 years diabetes duration. Most participants (84.7%) had established CVD or CKD at baseline. Following a relatively short follow up of 15.9 months, the primary composite endpoint of MACE was similar in the 2 groups; 3.8% in the semaglutide group and 4.8% in the placebo arm (HR 0.79; 95% CI 0.57-1.11), indicating CV safety but not demonstrating superiority as the trial was not designed to test this hypothesis. Death from CV causes was lower with semaglutide; 1.4% compared to 2.8% with placebo (HR 0.51; 95% CI, 0.31 to 0.84). This striking finding should be interpreted with care because of the small number of events and the short duration of follow up. In addition, due to the hierarchy of statistical testing, this result must only be considered exploratory. Based on these findings, the benefit of oral semaglutide to reduce the composite MACE outcome remains unproven.
Finally, the CV outcomes of albiglutide were evaluated in the Harmony Outcomes trial (9). Albiglutide was compared to placebo in 9,463 patients with type 2 diabetes and established CVD, and MACE occurred in 7% of albiglutide-treated patients and 9% of placebo-treated patients (HR 0.78, 95% 0.68-0.90) after a median 1.6 years, fulfilling criteria for noninferiority and superiority of albiglutide. Albiglutide is no longer marketed and is, therefore, not included as a potential treatment choice in this update.
Primary CV prevention in persons with CV risk factors
In contrast to most cardiovascular outcome trials (CVOT), which mainly included participants with a history of CV disease, the majority of participants in the Researching Cardiovascular Events With a Weekly Incretin in Diabetes (REWIND) trial (10) had CV risk factors only. This trial enrolled 9,901 participants with type 2 diabetes who were age ≥50 years and either had a previous CV event or age ≥60 years and at least 2 CV risk factors (hypertension, tobacco use, abdominal obesity or dyslipidemia), and they were randomized to subcutaneous dulaglutide (a GLP1-RA) 1.5 mg weekly or placebo. The mean age of participants was 66.2 years, median duration of diabetes was 9.5 years, the median A1C was 7.2% with 25% having a baseline A1C less than 6.6%, and 68.5% did not have CVD at baseline. After a median follow up of 5.4 years, there was a lower incidence of MACE with dulaglutide compared to placebo (12.0% vs 13.4%; HR 0.88, 95% CI 0.79-0.99; p=0.026). The hazard ratio was similar in those with and without previous CV disease. All-cause or CV mortality did not differ between groups. Since the majority of participants in the trial had CV risk factors rather than pre-existing CVD and many participants would be considered to be at target for A1C, this trial provides evidence for prevention of MACE with dulaglutide in people with type 2 diabetes without established ASCVD and in individuals who may be at A1C target.
In summary, there is substantial evidence that GLP1-RA (with the exception of lixisenatide) are associated with a significant reduction in risk of MACE among patients with type 2 diabetes and established CVD (11) (see also Table 2). The most reliable evidence for CV benefit from individual clinical trials is for liraglutide, dulaglutide and semaglutide. While CV safety has been confirmed for all GLP1-RA, there is no evidence of CV benefit for lixisenatide. The CV benefits of exenatide-ER and oral semaglutide remain unproven. Based on these findings, our recommendations have been updated to include dulaglutide and subcutaneous semaglutide as options for patients with ASCVD. We also now have evidence suggesting GLP1-RA, particularly dulaglutide, can reduce the risk of MACE in people without established CVD. This evidence has led to a recommendation that a GLP1-RA with proven CV outcome benefit can be considered in patients aged 60 years or older with at least 2 CV risk factors, with the strongest evidence for dulaglutide followed by liraglutide and subcutaneous semaglutide.
SGLT2i
Secondary CV prevention in persons with ASCVD
In 2018, empagliflozin and canagliflozin were included as options for patients with established CVD based on trials showing CV benefit; data regarding dapagliflozin were still pending. The Empagliflozin Cardiovascular Outcome Event Trial (EMPA-REG OUTCOME) randomized 7,020 participants with type 2 diabetes and clinical CVD to empagliflozin or placebo. After a median 3.1 years of follow up, those treated with empagliflozin had significantly fewer MACE compared to placebo-treated participants (10.5% vs 12.1%, HR 0.86, 95% CI 0.74-0.99). Empagliflozin was also associated with a significant decrease in CV mortality (HR 0.62, 95% CI 0.49-0.77) and in HHF (HR 0.65, 95% CI 0.50–0.85), but no reductions in nonfatal MI or stroke (12,13). As a prespecified component of the secondary composite microvascular outcome, progression of kidney disease was also lower in patients treated with empagliflozin vs placebo (12.7% vs 18.8%, HR 0.61, 95% CI 0.53-0.70) (14). The CV effects of canagliflozin were assessed in the Canagliflozin Cardiovascular Assessment Study (CANVAS) program, which integrated findings from 2 placebo-controlled trials (CANVAS and CANVAS-R) (15). The trials enrolled 10,142 participants (4,330 in CANVAS and 5,812 in CANVAS-R) with type 2 diabetes who were 30 years or older with symptomatic CVD (symptomatic ASCVD [coronary, cerebrovascular or peripheral] [66%]) or 50 years or older with at least 2 CV risk factors (34%). Over a median follow up of 2.4 years, canagliflozin-treated participants had significantly fewer MACE compared to placebo (26.9 vs 31.5 per 1,000 person-years; HR 0.86, 95% CI 0.75–0.97). There were no statistical differences in the individual components of the composite outcome. There was a reduction in HHF and in several adverse renal outcomes of similar magnitude to those seen in EMPA-REG; however, these outcomes were considered exploratory due to prespecified rules of hierarchy for statistical testing. While one-third of participants did not have CVD, a significant decrease in the primary endpoint was only found in those with CVD. In CANVAS, canagliflozin was associated with a higher risk of lower extremity amputation compared with placebo. Canagliflozin was not associated with an increased risk for amputations in the more recent CREDENCE trial (16).
Primary CV prevention in persons with CV risk factors
Since all EMPA-REG and the majority of CANVAS participants had ASCVD, the effects of SGLT2i on MACE in persons with type 2 diabetes without pre-existing CVD were unclear. The Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes trial (DECLARE TIMI 58) was the first SGLT2i CVOT to include a majority of patients with CV risk factors only (59%) (17) (see also Table 2). Patients with type 2 diabetes age 40 or older with established CVD, or age 55 or older for men and 60 or older for women with at least 1 CV risk factor (hypertension, dyslipidemia, tobacco use) were eligible to participate. This trial of 17,160 people was initially designed to test the safety of dapagliflozin on MACE. The protocol was then amended to include 2 primary efficacy outcomes: 1) MACE and 2) CV death or HHF. Participants had a mean age of 64 years, mean A1C of 8.3%, median duration of diabetes of 11 years and 41% had established ASCVD. Only 10% of participants had a history of heart failure (HF) at baseline. After a median follow up of 4.2 years, dapagliflozin met the pre-specified criterion for noninferiority compared to placebo for MACE but did not meet the criterion for superiority (8.8% vs 9.4%, HR 0.93 95% CI 0.84-1.03). There was a lower incidence of the other primary efficacy endpoint of CV death or HHF with dapagliflozin (4.9% vs 5.8%, HR 0.83 95% CI 0.73-0.95; p=0.005), which was driven by reduction of HHF. Dapagliflozin was also associated with a significant reduction in the secondary outcome of risk of kidney disease progression (4.3% vs 5.6%, HR 0.76, 95% CI 0.67-0.87). Although the incidence was rare, dapagliflozin was associated with a higher rate of diabetic ketoacidosis (0.3% vs 0.1%; HR 8.36; 95% CI 4.19-16.68; p<0.001). This trial included more than 10,000 participants with CV risk factors only, found no benefit for reduction of MACE, while expanding the evidence for the benefit of SGLT2i on reducing HHF and progression of kidney disease in this lower-risk group.
A meta-analysis of the above SGLT2i CVOT provides further evidence on the efficacy of SGLT2i on CV and renal outcomes in specific subgroups based on CV risk (18). This meta-analysis summarized the data from 34,322 participants, of which 20,650 (60.2%) had ASCVD and 13,672 (39.8%) had multiple CV risk factors only; 3,891 (11.3%) had a history of HF at baseline. First, SGLT2i were found to reduce the risk of MACE by 11% (HR 0.89 95% CI 0.83-0.96; p=0.0014). However, this beneficial effect was entirely restricted to those with ASCVD (HR 0.86, 95% CI 0.80-0.93) and no difference was found in those with multiple risk factors only (HR 1.00, 95% CI 0.87-1.16). Second, SGLT2i significantly reduced the risk for the composite of CV death or HHF (HR 0.77 95% CI 0.71-0.84; p<0.0001). In contrast to MACE, this benefit was shown for those with ASCVD (HR 0.76, 95% CI 0.69-0.84) and in those with multiple CV risk factors (HR 0.84, 95% 0.69-1.01). Third, SGLT2i were associated with a significant reduction in progression of kidney disease (composite of worsening renal function, end-stage renal disease or renal death) (HR 0.55 95% CI 0.48-0.64; p<0.0001). Again, similar to the effect on HHF, this effect was demonstrated both in people with ASCVD (HR 0.56, 95%CI 0.47-0.67) and in those with multiple CV risk factors (HR 0.54, 95% CI 0.42-0.71). These findings provide evidence to consider an SGLT2i in patients with multiple CV risk factors to reduce HHF and progression of nephropathy.
CV outcomes in persons with a history of HF
Previous CVOT have demonstrated that SGLT2i reduce the risk of HHF among persons who have type 2 diabetes, with and without pre-existing CVD (18). It should be noted, however, that only around 10% of participants had a history of HF at baseline in prior trials. In addition, with the exception of the DECLARE-TIMI trial, whereby the composite of HHF or CV death was included as a coprimary outcome (17), HHF was considered a secondary outcome.
The Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure (DAPA-HF) trial was the first trial of an SGLT2i to evaluate HF as a primary outcome in patients with HF (19). This trial randomized 4,744 people with New York Heart Association (NYHA) class II, III or IV HF and an ejection fraction ≤40% to dapagliflozin 10 mg daily or placebo in addition to recommended therapies for HF. Notably, the presence of diabetes was not an inclusion criteria and randomization was stratified based on the diagnosis of type 2 diabetes at baseline. Only 42% of participants had a diagnosis of type 2 diabetes at baseline and an additional 3% were diagnosed during the trial, making this the first CVOT to test SGLT2i in a population without diabetes. The primary outcome was a composite of worsening of HF (hospitalization or an urgent visit requiring IV therapy for HF) or CV death. Over a median of 18.2 months, the primary outcome occurred in 16.3% in the dapagliflozin group and 21.1% in the placebo group (HR 0.74, 95%CI 0.65-9.85; p<0.001). Dapagliflozin was associated with a lower risk for worsening HF (HR 0.70, 95% CI 0.59-0.83), CV death (HR 0.82 95%CI 0.69-0.98) and all-cause mortality (HR 0.83, 95% CI 0.71-0.97). The effect on the primary outcome was consistent across the prespecified subgroups of persons with and without type 2 diabetes at baseline. These findings provide evidence to recommend an SGLT2i in patients with HF to reduce the risk of HHF or CV death, with the strongest evidence for dapagliflozin from this trial, followed by canagliflozin and empagliflozin based on previous trials.
Cardiorenal outcomes in persons with CKD
SGLT2i have been shown to reduce progression of nephropathy as a secondary outcome in patients with CVD or with multiple CV risk factors (18). The Canagliflozin and Renal Endpoints in Diabetes with Established Nephropathy Clinical Evaluation (CREDENCE) study was the first trial to evaluate the effect of an SGLT2i on progression of kidney disease as a primary outcome in people with type 2 diabetes and established CKD with significant proteinuria (16). The trial randomized adults at least 30 years of age with type 2 diabetes, eGFR 30 to <90 mL/min/1.73m2 and albuminuria (urinary albumin:creatinine ratio >300 to 5,000 mg/g) receiving a stable dose of renin-angiotensin system blockade, to canagliflozin 100 mg daily or placebo. The primary composite endpoint of kidney disease progression was end-stage kidney disease (dialysis, transplantation or sustained eGFR <15 mL/min/1.73m2), doubling of serum creatinine, and renal or CV death. The trial was stopped early after a planned interim analysis indicated that reduced risk for the primary outcome had been demonstrated. At that time, 4,401 people had been randomized with a median follow up of 2.62 years. The mean age was 63 years, mean A1C was 8.3%, mean eGFR was 56.2 mL/min/1.73m2 with a median urinary albumin:creatinine ratio of 927 mg/g. The relative risk of the primary outcome was 30% lower in the canagliflozin group compared to placebo, with event rates of 43.2 and 61.2 per 1,000 patient years (HR 0.70; 95% CI 0.59-0.82; p=0.00001). The canagliflozin group also had a lower risk of the secondary outcome of MACE (HR 0.80; 95% CI, 0.67 to 0.95; p=0.01) and HHF (HR 0.61; 95% CI, 0.47 to 0.80; p<0.001). There were no significant differences in rates of amputation or fracture, both of which had been noted with canagliflozin in the CANVAS trial. There was a higher rate of diabetic ketoacidosis with canagliflozin, although the rate was relatively low (2.2 vs 0.2 per 1,000 patient years). This trial supports a recommendation for an SGLT2i in patients with CKD and eGFR >30 mL/min/1.73m2 to reduce their risk of kidney disease progression, with the strongest evidence for canagliflozin, followed by dapagliflozin and empagliflozin.
Two GLP1-RA have also been shown to reduce MACE outcomes specifically in patients with type 2 diabetes and CKD. In LEADER, the benefits of liraglutide on MACE appeared to be greatest in the 23% of patients with at least moderate CKD (eGFR <60 mL/min/1.73m2) (HR for CKD 0.69, 95% CI 0.57 to 0.85 and no CKD 0.94, 95% 0.83 to 1.07; p=0.01 for interaction) (6). In SUSTAIN-6, 28% of participants had CKD and the benefits of subcutaneous semaglutide were comparable to those without CKD (7). These agents may, therefore, be considered in patients with CKD to reduce the risk of MACE.
DPP4i
Five DPP4i CVOT have been completed; 2 additional CVOT of linagliptin (comparing to placebo or glimepiride) were published since the 2018 guidelines (see Table 2). No DPP4i has shown inferiority or superiority compared to placebo for the risk of major CV events (20-23). This was also true for linagliptin when compared with glimepiride. Saxagliptin was associated with an increased incidence of HHF (21) that has yet to be fully explained and, therefore, this agent is not recommended in people with a history of HF, with CV disease or multiple CV risk factors.
Summary of CV benefits and risks of antihyperglycemic agents
Most recently, Zhu et al conducted an umbrella review of randomized controlled trials to summarize evidence regarding the association between antihyperglycemic medications and CV outcomes (24). This review confirmed previous evidence that several GLP1-RA and SGLT2i showed CV outcome benefits, including reducing the risk of major adverse CV events (dulaglutide, liraglutide, semaglutide, canagliflozin, empagliflozin), death (canagliflozin, empagliflozin), MI (dulaglutide, exenatide, liraglutide, semaglutide), HF (canagliflozin, dapagliflozin, empagliflozin) and stroke (dulaglutide). Notably, some medications also increased the risk of CV outcomes, including increasing the risk of HF (saxagliptin, rosiglitazone, pioglitazone), MI (rosiglitazone) and stroke (glimepiride). Pioglitazone was associated with both harms and benefits, including an increased risk of HF but a decreased risk of major adverse CV events, MI and stroke. Several classes of medications were found to be neutral with confirmed CV safety, including insulin, DPP4i, meglitinides and dopamine agonists. This review confirms findings from individual trials and supports current recommendations, and provides evidence to recommend against the use of thiazolidinediones (TZD) and saxagliptin for patients with HF. Although metformin has not been formally evaluated in a CVOT, all of the trials in type 2 diabetes patients have been conducted on a background of metformin.
It should also be noted that all type 2 diabetes CVOT have been conducted in patients with established type 2 diabetes on existing antihyperglycemic therapy. We, therefore, do not have clinical trial evidence for cardiorenal benefits of GLP1-RA and SGLT2i in patients with newly diagnosed type 2 diabetes. However, given the totality of evidence to date, it is likely that these benefits can be extrapolated to newly diagnosed patients WITH ASCVD, history of HF and/or CKD. However, in the absence of clinical trial data, we have not added a recommendation, but have discussed this scenario in the accompanying commentary document (25).
Comparative effectiveness of antihyperglycemic agents
For patients without CVD in whom glycemic targets are not achieved on their current antihyperglycemic therapy, the 2018 guidelines recommended incretin agents (DPP4i or GLP1-RA) and/or SGLT2i over insulin secretagogues, insulin and TZD to improve glycemic control if lower risk of hypoglycemia and/or weight gain were priorities. This recommendation was based on meta-analyses that summarized head-to-head comparisons of metformin-based combinations (26-30). For glycemic control, these studies showed that combinations of metformin with a sulfonylurea, TZD, SGLT2i, DPP4i or GLP1-RA have broadly comparable A1C-lowering benefits (26,27,28,29,31-33). Theoretically, insulin does not have a dose limit and would be expected to have the greatest potential for A1C lowering (although dose increases may be limited by hypoglycemia and higher doses of insulin can become expensive). In contrast, agents were shown to have differential effects on risk of hypoglycemia and weight change. The risk of hypoglycemia is lower with TZD, DPP4i, SGLT2i and GLP1-RA compared to sulfonylureas and insulin (26-29,31,32,34,35). For weight, TZD, insulin and sulfonylureas are associated with the most weight gain (1.5 to 5.0 kg), DPP4i have a neutral effect on weight, and GLP1-RA and SGLT2i lead to weight loss. Prescribers should remember that the mean differences reported in short duration phase 3 trials may not accurately predict the response of an individual patient. Responses to some drugs are also subject to large degrees of interindividual variation, particularly with respect to changes in weight and A1C.
Additional head-to-head trials have since been published that confirm these findings and provide stronger evidence for weight-loss benefits of GLP1-RA and SGLT2i (30). We also have evidence of primary CV prevention for certain GLP1-RA and of prevention of HF for SGLT2i in patients with multiple CV risk factors, as outlined above. We have, therefore, made 2 changes to the recommendation for antihyperglycemic agent selection in patients without CVD. First, a GLP1-RA and/or an SGLT2i with proven CV benefit is recommended for persons aged 60 or older with at least 2 CV risk factors. Second, to acknowledge differing effects of agents on risk of hypoglycemia and weight loss, we have revised our recommendation to consider the priorities of avoiding hypoglycemia and weight gain separately. For patients requiring antihyperglycemic treatment optimization in whom reducing risk of hypoglycemia is a priority, an incretin agent (DPP4i or GLP1-RA), an SGLT2i and/or pioglitazone should be considered as add-on therapy before an insulin secretagogue (sulfonylurea or meglitinide) or insulin due to their lower risk of hypoglycemia. For those in whom weight loss is a priority, a GLP1-RA and/or an SGLT2i should be considered as first options for add-on therapy as they are associated with significantly greater weight loss than other antihyperglycemic agents.
Summary
The rapid release of evidence over the last few years from trials of antihyperglycemic agents has led to an important shift in treatment decisions that were based solely on glycemic effects to now include potential benefits on other clinically relevant outcomes. Based on a careful review of this evidence, the updated recommendations provide more specific treatment guidance for clinicians and people living with type 2 diabetes. We now have more evidence to recommend certain agents over others for patients with CVD, a history of HF, CKD and in those 60 years or older with multiple CV risk factors. As always, treatment decisions need to be individualized, considering a patient’s needs and preferences, access and cost, and degree of glucose-lowering needed.
RECOMMENDATIONS
Treatment of People With Newly Diagnosed Type 2 Diabetes (see Figure 1)
- Healthy behaviour interventions should be initiated at type 2 diabetes diagnosis [Grade B, Level 2 (36)] and reinforced and maintained throughout. Metformin may be introduced at the time of diagnosis, in conjunction with healthy behaviour interventions [Grade D, Consensus].
- If glycemic targets are not achieved within 3 months using healthy behaviour interventions alone, antihyperglycemic therapy should be added to reduce the risk of microvascular complications [Grade A, Level 1A (37)]. Metformin should usually be selected before other agents due to its low risk of hypoglycemia and weight gain [Grade A, Level 1A (26)], and long-term experience with this agent [Grade D, Consensus].
- If A1C values are ≥1.5% above target, initiating metformin in combination with a second antihyperglycemic agent should be considered to increase the likelihood of reaching target [Grade B, Level 2 (38-40) for SGLT2i (41); for DPP4i (42,43)].
- Individuals with metabolic decompensation (e.g. marked hyperglycemia, ketosis or unintentional weight loss) should receive insulin with or without metformin, until glycemic control is achieved OR type of diabetes is established [Grade D, Consensus].
Reassessment and Monitoring
- Glycemic control, cardiovascular and renal status should be reviewed regularly (at least annually). Healthy behaviour interventions should be reinforced and supported. Efficacy, side effects and adherence to existing antihyperglycemic therapy should be assessed [Grade D, Consensus].
- Dose adjustments, substitutions and/or addition of antihyperglycemic medications should be made in order to maintain A1C or attain target A1C within 3 to 6 months [Grade D, Consensus].
- If glycemic targets are not achieved with existing antihyperglycemic medication(s), or the individual’s clinical status changes, other classes of agents should be used (either by addition or replacement) to reduce cardiorenal outcomes and/or improve glycemic control; or glycemic targets should be reassessed [Grade D, Consensus].
- For adults with type 2 diabetes with metabolic decompensation (e.g. marked or symptomatic hyperglycemia, ketosis or unintentional weight loss), insulin should be used (see #12-16, below) [Grade D, Consensus].
Advancement or Adjustment of Treatment in People With Type 2 Diabetes
- In adults with type 2 diabetes WITH ASCVD, HF and/or CKD, treatment should include agents from the following classes with demonstrated CV or renal benefits (see Figures 2A, 2B and Table 2).
- In adults with type 2 diabetes and ASCVD, a GLP1-RA or SGLT2i with CV or renal benefit should be used to reduce the risk of:
- MACE [Grade A, Level 1A (6,10) for liraglutide and dulaglutide; Grade B, Level 2 for subcutaneous semaglutide (7); Grade A, Level 1A (12) for empagliflozin; Grade B, Level 2 (15) for canagliflozin].
- HHF [Grade B, Level 2 (12,15,17) for empagliflozin, canagliflozin and dapagliflozin].
- Progression of nephropathy [Grade B, Level 2 (44,15,17) for empagliflozin, canagliflozin and dapagliflozin].
- In adults with type 2 diabetes and a history of HF (reduced ejection fraction ≤40%):
- An SGLT2i should be used to reduce the risk of HHF or CV death, if the eGFR is >30 mL/min/1.73m2 [Grade A, Level 1A (19) for dapagliflozin; Grade A, Level 1 (18) for empagliflozin and canagliflozin].
- TZD and saxagliptin should be avoided due to their higher risk of HF [Grade A, Level 1A (21,45,46)].
- In adults with type 2 diabetes and CKD and an estimated eGFR >30 mL/min/1.73m2:
- In adults with type 2 diabetes and ASCVD, a GLP1-RA or SGLT2i with CV or renal benefit should be used to reduce the risk of:
- In adults with type 2 diabetes requiring treatment advancement or adjustment to improve glycemic control, the choice of antihyperglycemic medication should be individualized according to clinical priorities (see Figure 2A and Table 1 for therapeutic considerations and cautions) [Grade B, Level 2 (26)].
- In adults with type 2 diabetes aged 60 years or older with at least 2 CV risk factors (see Table 3
- A GLP1-RA with proven CV outcome benefit to reduce the risk of MACE [Grade A, Level 1A (10) for dulaglutide; Grade B, Level 2 (6) for liraglutide and Grade C, Level 2 (7) subcutaneous semaglutide]; OR
- An SGLT2i with proven cardiorenal outcome benefit if estimated GFR is >30 mL/min/1.73m2 to reduce the risk of
- If reducing risk of hypoglycemia is a priority: Incretin agents (DPP4i or GLP1-RA), SGLT2i, acarbose and/or pioglitazone should be considered as add-on medication to improve glycemic control with a lower risk of hypoglycemia than other agents [Grade A, Level 1A (26,28,29,47,48,49,74)]. (See Table 1.)
- If weight loss is a priority: A GLP1-RA and/or SGLT2i should be considered as add-on medication to improve glycemic control with more weight loss than other agents [Grade A, Level 1A (26,28,29,30,47,48,49]. (See Table 1.)
- In adults with type 2 diabetes aged 60 years or older with at least 2 CV risk factors (see Table 3
Initiating Insulin Treatment in Patients With Type 2 Diabetes
- In people not achieving glycemic targets on existing noninsulin antihyperglycemic medication(s), the addition of a basal insulin regimen should be considered over premixed insulin or bolus-only regimens, if lower risk of hypoglycemia and/or preventing weight gain are priorities [Grade B, Level 2 (50)].
- In adults with type 2 diabetes treated with basal insulin therapy, if minimizing risk of hypoglycemia is a priority:
- Long-acting insulin analogues (insulin glargine U-100, glargine U-300, detemir, degludec) should be considered over NPH insulin to reduce the risk of nocturnal and symptomatic hypoglycemia [Grade A, Level 1A (51-56)].
- Insulin degludec or insulin glargine U-300 (57) may be considered over insulin glargine U-100 to reduce overall and nocturnal hypoglycemia [Grade B, Level 2 for individuals with ≥1 risk factor for hypoglycemia (58,59)]; [Grade C, Level 3 for other individuals without risk factors for hypoglycemia (56)]; and severe hypoglycemia in patients at high CV risk [Grade C, Level 3 (60)]
Treatment Advancement or Adjustment for People With Type 2 Diabetes Treated With Insulin
- In adults with type 2 diabetes receiving insulin, doses should be adjusted and/or additional antihyperglycemic medication(s) should be added if glycemic targets are not achieved [Grade D, Consensus].
- A GLP1-RA should be considered as add-on therapy [Grade A, Level 1A (61,62)], before initiating bolus insulin or intensifying insulin to improve glycemic control with potential benefits of weight loss and lower hypoglycemia risk compared to single or multiple bolus insulin injections [Grade A, Level 1A (63-71)].
- An SGLT2i should be considered as add-on therapy to improve glycemic control with potential benefits of weight loss and lower hypoglycemia risk compared to additional insulin [Grade A, Level 1A (72-74)].
- A DPP4i may be considered as add-on therapy to improve glycemic control with potential benefits of less weight gain and lower hypoglycemia risk compared to additional insulin [Grade B, Level 2 (72,75-77)].
- When bolus insulin is added to antihyperglycemic agents, rapid-acting analogues may be considered over short-acting (regular) insulin for greater improvement in glycemic control [Grade B, Level 2 (78,79) for aspart].
- Bolus insulin may be initiated using a stepwise approach (starting with 1 injection at 1 meal and additional mealtime injections as needed) to achieve similar A1C reduction with lower hypoglycemia risk compared to initiating bolus injections at every meal [Grade B, Level 2 (80)].
Safety Considerations for Pharmacotherapy of Type 2 Diabetes
- All individuals with type 2 diabetes currently using or starting therapy with insulin or insulin secretagogues should be counselled about the prevention, recognition and treatment of hypoglycemia [Grade D, Consensus].
- Pharmacotherapy may need to be temporarily adjusted during acute illness or around the time of some investigations:
- Metformin and SGLT2i should be temporarily withheld during acute illnesses associated with risk for dehydration or procedures associated with high risk of acute kidney injury [Grade D, Consensus]. (See Appendix 8. Sick-Day Medication List. 2018 CPG.)
- Insulin and insulin secretagogue doses should be decreased or held to reduce risk for hypoglycemia if oral intake is reduced [Grade D, Consensus]. (See Appendix 8. Sick-Day Medication List. 2018 CPG.)
- SGLT2i should be temporarily withheld prior to major surgical procedures and during acute infections and serious illness to reduce the risk of ketoacidosis [Grade D, Consensus]. Particular caution should be paid to this risk in people following low-carbohydrate eating patterns (81) or with suspected insulin deficiency [Grade D, Consensus].
Author Disclosures
Dr. Senior reports no personal fees for speaking, consulting or clinical trials for industry partners since 2018, but is a local Principal Investigator for clinical trials sponsored by Novo Nordisk at the University of Alberta and is in compliance with institutional policies governing interactions with industry. He reports research support from the American Diabetes Association, the Juvenile Diabetes Research Foundation, the National Institutes of Health, and salary support from the Alberta Academic Medicine and Health Services Plan. He is also a member of the Diabetes Canada Board of Directors. Dr. Lipscombe reports salary support from a Diabetes Canada Diabetes Investigator Award. Dr. MacCallum reports personal fees from Janssen, Novo Nordisk, grants from Eli Lilly and Merck, and her spouse is an employee at Johnson and Johnson. She is in compliance with the University of Toronto’s policies governing interactions with industry. No other authors have any disclosures.
References
- Diabetes Canada Clinical Practice Guidelines Expert Committee. Diabetes Canada 2018 Clinical practice guidelines for the prevention and management of diabetes in Canada. Can J Diabetes 2018;42(suppl 1):S1e325.
- Houlden RL. Diabetes Canada 2018 Clinical practice guidelines for the pre- vention and management of diabetes in Canada: Introduction. Can J Diabetes 2018;42(Suppl 1):S1e5.
- Sherifali D, Rabi D, Houlden RL. Diabetes Canada 2018 Clinical practice guidelines for the prevention and management of diabetes in Canada: Methods. 2018;42(Suppl 1):S6e9.
- Pfeffer MA, Claggett B, Diaz R, et al. Lixisenatide in patients with type 2 diabetes and acute coronary syndrome. N Engl J Med 2015;373:2247e57.
- Holman RR, Bethel MA, Mentz RJ, et al; the EXSCEL Study Group. Effects of Once-Weekly Exenatide on Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med 2017;377:1228e39.
- Marso SP, Daniels GH, Brown-Frandsen K, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2016;375:311e22.
- Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med 2016;375:1834e44.
- Husain M, Birkenfeld AL, Donsmark M, et al; the PIONEER 6 Investigators. Oral semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med 2019;381:841e51.
- Hernandez AF, Green JB, Janmohamed S, et al; Harmony Outcomes Com- mittees and Investigators. Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Out- comes): A double-blind, randomised placebo-controlled trial. Lancet 2018; 392:P1519e29.
- Gerstein HC, Colhoun HM, Dagenais GR, et al; REWIND Investigators. Dula- glutide and cardiovascular outcomes in type 2 diabetes (REWIND): A double- blind, randomised placebo-controlled trial. The Lancet 2019;394:121e30.
- Kristensen SL, Rørth R, Jhund PS, et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: A systematic review and meta-analysis of cardiovascular outcome trials. Lancet Diabetes Endocrinol 2019;7:776e85.
- Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 2015;373:2117e28.
- Fitchett D, Zinman B, Wanner C, et al. Heart failure outcomes with empagli- flozin in patients with type 2 diabetes at high cardiovascular risk: Results of the EMPA-REG OUTCOME trial. Eur Heart J 2016;37:1526e34.
- Wanner C, Inzucchi SE, Lachin JM, et al; the EMPA-REG OUTCOME Investiga- tors. Empagliflozin and Progression of Kidney Disease in Type 2 Diabetes. N Engl J Med 2016;375:323e34.
- Neal B, Perkovic V, Mahaffey KW, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med 2017;377:644e57.
- Perkovic V, Jardine MJ, Neal B, et al; Credence Trial Investigators. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med 2019; 380(24):2295e306.
- Wiviott SD, Raz I, Bonaca MP, et al; Declare-Timi Investigators. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2019;380: 347e57.
- ZelnikerTA,WiviottSD,RazI,etal.SGLT2inhibitorsforprimaryandsecondary prevention of cardiovascular and renal outcomes in type 2 diabetes: A sys- tematic review and meta-analysis of cardiovascular outcome trials. The Lancet 2019;393:31e9.
- McMurray JJV, Solomon SD, Inzucchi SE, et al; the DAPA-HF Trial Committees and Investigators. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N Engl J Med 2019;381:1995e2008.
- White WB, Cannon CP, Heller SR, et al. Alogliptin after acute coronary syn- drome in patients with type 2 diabetes. N Engl J Med 2013;369:1327e35.
- Scirica BM, Bhatt DL, Braunwald E, et al. Saxagliptin and cardiovascular out- comes in patients with type 2 diabetes mellitus. N Engl JMed 2013;369: 1317e26.
- Rosenstock J, Kahn SE, Johansen OE, et al; Carolina Investigators. Effect of linagliptin vs glimepiride on major adverse cardiovascular outcomes in patients with type 2 diabetes: The CAROLINA randomized clinical trial. JAMA 2019;322:1155e66.
- Rosenstock J, Perkovic P, Johansen OE, et al; Carmelina Investigators. Effect of linagliptin vs placebo on major cardiovascular events in adults with type 2 diabetes and high cardiovascular and renal risk: The CARMELINA randomized clinical trial. JAMA 2019;321:69e79.
- Zhu J, Yu X, Zheng Y, et al. Association of glucose-lowering medications with cardiovascular outcomes: An umbrella review and evidence map. Lancet Dia- betes Endocrinol 2020;8:192e205.
- Senior PA, Houlden RL, Kim J, et al. Pharmacologic glycemic management of type 2 diabetes in adults: 2020 update - the user’s guide. Can J Diabetes 2020; 44:589e93.
- Maruthur NM, Tseng E, Hutfless S, et al. Diabetes medications as monotherapy or metformin-based combination therapy for type 2 diabetes: A systematic review and meta-analysis. Ann Intern Med 2016;164:740e51.
- Mearns ES, Sobieraj DM, White CM, et al. Comparative efficacy and safety of antidiabetic drug regimens added to metformin monotherapy in patients with type 2 diabetes: A network meta-analysis. PLoS ONE 2015;10: e0125879.
- Mishriky BM, Cummings DM, Tanenberg RJ. The efficacy and safety of DPP4 inhibitors compared to sulfonylureas as add-on therapy to metformin in patients with type 2 diabetes: A systematic review and meta-analysis. Diabetes Res Clin Pract 2015;109:378e88.
- Foroutan N, Muratov S, Levine M. Safety and efficacy of dipeptidyl peptidase-4 inhibitors vs sulfonylurea in metformin-based combination therapy for type 2 diabetes mellitus: Systematic review and meta-analysis. Clin Invest Med 2016; 39:E48e62.
- Andreadis P, Karagiannis T, Malandris K, et al. Semaglutide for type 2 diabetes mellitus: A systematic review and meta-analysis. Diabetes Obes Metab 2019; 20:2255e63.
- Clar C, Gill JA, Court R, et al. Systematic review of SGLT2 receptor inhibitors in dual or triple therapy in type 2 diabetes. BMJ Open 2012;2:e001007.
- Hartley P, Shentu Y, Betz-Schiff P, et al. Efficacy and tolerability of sitagliptin compared with glimepiride in elderly patients with type 2 diabetes mellitus and inadequate glycemic control: A randomized, double-blind, non-inferiority trial. Drugs Aging 2015;32:469e76.
- Zhong X, Lai D, Ye Y, et al. Efficacy and safety of empagliflozin as add-on to metformin for type 2 diabetes: A systematic review and meta-analysis. Eur J Clin Pharmacol 2016;72:655e63.
- Schopman JE, Simon AC, Hoefnagel SJ, et al. The incidence of mild and severe hypoglycaemia in patients with type 2 diabetes mellitus treated with sulfo- nylureas: A systematic review and meta-analysis. Diabetes Metabolism Res Rev 2014;30:11e22.
- KimSS,KimIJ,LeeKJ,etal.Efficacyandsafetyofsitagliptin/metforminfixed-dose combination compared with glimepiride in patients with type 2 diabetes: A multicenter randomized double-blind study. J Diabetes 2016;9:412e22.
- Gregg EW, Chen H, Wagenknecht LE, et al. Association of an intensive lifestyle intervention with remission of type 2 diabetes. JAMA 2012;308: 2489e96.
- UKProspectiveDiabetesStudy(UKPDS)Group.Intensiveblood-glucosecontrol with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998;352:837e53.
- Phung OJ, Sobieraj DM, Engel SS, et al. Early combination therapy for the treatment of type 2 diabetes mellitus: Systematic review and meta-analysis. Diabetes Obes Metab 2014;16:410e7.
- RosenstockJ,ChuckL,Gonzalez-OrtizM,etal.Initialcombinationtherapywith canagliflozin plus metformin versus each component as monotherapy for drug naive type 2 diabetes. Diabetes Care 2016;39:353e62.
- Gao W, Dong J, Liu J, et al. Efficacy and safety of initial combination of DPP-IV inhibitors and metformin versus metformin monotherapy in type 2 diabetes: A systematic review of randomized controlled trials. Diabetes Obes Metab 2014; 16:179e85.
- Milder TY, Stocker SL, Shaheed CA, et al. Combination therapy with an SGLT2 inhibitor as initial treatment for type 2 diabetes: A systematic review and meta-analysis. J Clin Med 2019;8:45.
- Matthews DR, Paldánius PM, Proot P, et al. Glycaemic durability of an early combination therapy with vildagliptin and metformin versus sequential metformin monotherapy in newly diagnosed type 2 diabetes (VERIFY): A 5-year, multicentre, randomised, double-blind trial. The Lancet 2019;394:1519e29.
- Frias JP, Zimmer Z, Lam RLH, et al. Double-blind, randomized clinical trial assessing the efficacy and safety of early initiation of sitagliptin during metformin uptitration in the treatment of patients with type 2 diabetes: The CompoSIT-M study. Diabetes Obes Metab 2019;21:1128e35.
- Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and progression of kidney disease in type 2 diabetes. N Engl J Med 2016;375:323e34.
- Wallach JD, Wang K, Zhang AD, et al. Updating insights into rosiglitazone and cardiovascular risk through shared data: Individual patient and summary level meta-analyses. BMJ 2020;368:l7078.
- Zhu J, Yu X, Zheng Y, et al. Association of glucose-lowering medications with cardiovascular outcomes: An umbrella review and evidence map. Lancet Dia- betes Endocrinol 2020;8:192e205.
- LiuSC,TuYK,ChienMN,etal.Effectofantidiabeticagentsaddedtometformin on glycaemic control, hypoglycaemia and weight change in patients with type 2 diabetes: A network meta-analysis. Diabetes Obes Metab 2012;14: 810e20.
- Zhou JB, Bai L, Wang Y, et al. The benefits and risks of DPP4-inhibitors vs. sulfonylureas for patients with type 2 diabetes: Accumulated evidence from randomised controlled trial. Int J Clin Pract 2016;70:132e41.
- McIntosh B, Cameron C, Singh SR, et al. Choice of therapy in patients with type 2 diabetes inadequately controlled with metformin and a sulphonylurea: A systematic review and mixed-treatment comparison meta-analysis. Open Med 2012;6:e62e74.
- Holman RR, Farmer AJ, Davies MJ, et al. Three-year efficacy of complex insulin regimens in type 2 diabetes. N Engl J Med 2009;361:1736e47.
- Zinman B, Philis-Tsimikas A, Cariou B, et al. Insulin degludec versus insulin glargine in insulin-naive patients with type 2 diabetes: A 1-year, randomized, treat-to-target trial (BEGIN Once Long). Diabetes Care 2012;35:2464e71.
- Singh SR, Ahmad F, Lal A, et al. Efficacy and safety of insulin analogues for the management of diabetes mellitus: A meta-analysis. CMAJ 2009;180: 385e97.
- Horvath K, Jeitler K, Berghold A, et al. Long-acting insulin analogues versus NPH insulin (human isophane insulin) for type 2 diabetes mellitus. Cochrane Database Syst Rev 2007;(2):CD005613.
- Monami M, Marchionni N, Mannucci E. Long-acting insulin analogues versus NPH human insulin in type 2 diabetes: Ameta-analysis. Diabetes Res Clin Pract 2008;81:184e9.
- Rys P, Wojciechowski P, Rogoz-Sitek A, et al. Systematic review and meta- analysis of randomized clinical trials comparing efficacy and safety outcomes of insulin glargine with NPH insulin, premixed insulin preparations or with insulin detemir in type 2 diabetes mellitus. Acta Diabetol 2015;52: 649e62.
- Ratner RE, Gough SC, Mathieu C, et al. Hypoglycaemia risk with insulin degludec compared with insulin glargine in type 2 and type 1 diabetes: A pre- planned meta-analysis of phase 3 trials. Diabetes Obes Metab 2013;15:175e84.
- Rosenstock J, Cheng A, Ritzel R, et al. More similarities than differences testing insulin glargine 300 units/mL versus insulin degludec 100 units/mL in insulin- naive type 2 diabetes: The randomized head-to-head BRIGHT trial. Diabetes Care 2018;41:2147e54.
- Wysham C, Bhargava A, Chaykin L, et al. Effect of insulin degludec vs insulin glargine U100 on hypoglycemia in patients with type 2 diabetes. The SWITCH 2 Randomized Clinical Trial. JAMA 2017;318:45e56.
- Heller SR, DeVries JH, Wysham C, et al. Lower rates of hypoglycaemia in older individuals with type 2 diabetes using insulin degludec versus insulin glargine U100: Results from SWITCH 2. Diabetes Obes Metab 2019;21:1634e41.
- Marso SP, McGuire DK, Zinman B, et al. Efficacy and safety of degludec versus glargine in type 2 diabetes. N Engl J Med 2017;377:723e32.
- Buse JB, Bergenstal RM, Glass LC, et al. Use of twice-daily exenatide in basal insulin-treated patients with type 2 diabetes: A randomized, controlled trial. Ann Intern Med 2011;154:103e12.
- Ahmann A, Rodbard HW, Rosenstock J, et al. Efficacy and safety of liraglutide versus placebo added to basal insulin analogues (with or without metformin) in patients with type 2 diabetes: A randomized, placebo-controlled trial. Dia- betes Obes Metab 2015;17:1056e64.
- Mathieu C, Rodbard HW, Cariou B, et al. A comparison of adding liraglutide versus a single daily dose of insulin aspart to insulin degludec in subjects with type 2 diabetes (BEGIN: VICTOZA ADD-ON). Diabetes Obes Metab 2014;16:636e44.
- Rosenstock J, Guerci B, Hanefeld M, et al. Prandial options to advance basal insulin glargine therapy: Testing lixisenatide plus basal insulin versus insulin glulisine either as basal-plus or basal-bolus in type 2 diabetes: The GetGoal Duo-2 Trial. Diabetes Care 2016;39:1318e28.
- Eng C, Kramer CK, Zinman B, et al. Glucagon-like peptide-1 receptor agonist and basal insulin combination treatment for the management of type 2 diabetes: A systematic review and meta-analysis. Lancet 2014;384:2228e34.
- Maiorino MI, Chiodini P, Bellastella G, et al. Insulin and Glucagon-Like Peptide 1 Receptor Agonist Combination Therapy in Type 2 Diabetes: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Diabetes Care 2017;40:614e24.
- Wysham CH, Lin J, Kuritzky L. Safety and efficacy of a glucagon-like peptide-1 receptor agonist added to basal insulin therapy versus basal insulin with or without a rapid-acting insulin in patients with type 2 diabetes: Results of a meta-analysis. Postgraduate Medicine 2017;129:436e45.
- Pozzilli P, Norwood P, Jodar E, et al. Placebo-controlled, randomized trial of the addition of once-weekly glucagon-like peptide-1 receptor agonist dulaglutide to titrated daily insulin glargine in patients with type 2 diabetes (AWARD-9). Diabetes Obes Metab 2017;19:1024e31.
- Rodbard HW, Lingvay I, Reed J, et al. Semaglutide added to basal insulin in type 2 diabetes (SUSTAIN 5): A randomized, controlled trial. J Clin Endocrinol Metab 2018;103:2291e301.
- Aroda VR, Bain SC, Cariou B, et al. Efficacy and safety of once-weekly semaglutide versus once-daily insulin glargine as add-on to metformin (with or without sulfonylureas) in insulin-naive patients with type 2 diabetes (SUSTAIN 4): A randomised, open-label, parallel-group, multicentre, multinational, phase 3a trial. Lancet Diabetes Endocrinol 2017;5:355e66.
- Billings LK, Doshi A, Gouet D, et al. Efficacy and safety of IDegLira versus basal- bolus insulin therapy in patients with type 2 diabetes uncontrolled on met- formin and basal insulin: DUAL VII randomized clinical trial. Diabetes Care 2018;41:1009e16.
- Min SH, Yoon JH, Hahn S, et al. Comparison between SGLT2 inhibitors and DPP4 inhibitors added to insulin therapy in type 2 diabetes: A systematic review with indirect comparison meta-analysis. Diabetes Metab Res Rev 2016;33: e2818.
- Rosenstock J, Jelaska A, Frappin G, et al. Improved glucose control with weight loss, lower insulin doses, and no increased hypoglycemia with empagliflozin added to titrated multiple daily injections of insulin in obese inadequately controlled type 2 diabetes. Diabetes Care 2014;37:1815e23.
- Wilding JP, Woo V, Rohwedder K, et al. Dapagliflozin in patients with type 2 diabetes receiving high doses of insulin: Efficacy and safety over 2 years. Diabetes Obes Metab 2014;16:124e36.
- Zinman B, Ahren B, Neubacher D, et al. Efficacy and cardiovascular safety of linagliptin as an add-on to insulin in type 2 diabetes: A pooled comprehensive post hoc analysis. Can J Diabetes 2016;40:50e7.
- Kesavadev J, Sadasivan Pillai Pradeep Babu, Shankar A, et al. Sitagliptin 100 mg vs glimepiride 1-3 mg as an add-on to insulin and metformin in type 2 diabetes (SWIM). Endocrine Connections 2017;6:748e57.
- Ledesma G, Umpierrez GE, Morley JE, et al. Efficacy and safety of linagliptin to improve glucose control in older people with type 2 diabetes on stable insulin therapy: A randomized trial. Diabetes Obes Metab 2019;21: 2465e73.
- Mannucci E, Monami M, Marchionni N. Short-acting insulin analogues vs. regular human insulin in type 2 diabetes: A meta-analysis. Diabetes Obes Metab 2009;11:53e9.
- Bowering K, Case C, Harvey J, et al. Faster aspart versus insulin sspart as part of a basal-bolus regimen in inadequately controlled type 2 diabetes: The onset 2 trial. Diabetes Care 2017;40:951e7.
- Rodbard HW, Visco VE, Andersen H, et al. Treatment intensification with stepwise addition of prandial insulin aspart boluses compared with full basal- bolus therapy (FullSTEP Study): A randomised, treat-to-target clinical trial. Lancet Diabetes Endocrinol 2014;2:30e7.
- Diabetes Canada position statement on low-carbohydrate diets for adults with diabetes: A rapid review. Can J Diabetes 2020;44:295e9.
Diabetes Canada is the registered owner of all content on guidelines.diabetes.ca and ShopDC. For questions, please email info@diabetes.ca