Chapter Headings
- Key Messages
- Key Messages for People With Diabetes
- Introduction
- Psychological Adaptation/Expectable Reactions to the Diagnosis of Diabetes
- Established Psychological Syndromes Related to the Diagnosis of Diabetes
- Summary of Psychological Syndromes Associated With Diabetes
- Distinguishing Diabetes Distress From Major Depressive Disorder
- Stigma: Comorbid Diabetes and Mental Health Issues
- Financial Burden/Financial Distress of Diabetes
- Psychiatric Conditions in Adults
- Psychiatric Disorders and Adverse Outcomes
- Children and Adolescents
- Considerations for Older People With Diabetes
- Recreational Substance Use
- COVID-19 and Mental Health
- Screening and Assessment of Mental Health in Diabetes
- Pharmacological Treatments
- Antidepressant Medications
- Monitoring Metabolic Risks
- Recommendations
- Author Disclosures
- Acknowledgments
Key Messages
Living With Diabetes
- The diagnosis and management of diabetes can be a significant life stressor for individuals and their families, and may be associated with challenges regarding illness acceptance and treatment participation. Addressing concerns regarding illness beliefs and participation in treatment recommendations can be helpful.
- The lived experience of diabetes is often associated with struggles specific to the illness and can lead to significant concerns, specifically diabetes distress, perpetuation of stigma, reluctance to initiate insulin when recommended, and the persistent fear of hypoglycemic episodes.
Psychological Reactions to the Diagnosis of Diabetes
- Well-established reactions to diabetes include: perceptions about the seriousness of the disease (either discounting the seriousness of diabetes, which is often seen in those with asymptomatic type 2 diabetes [T2D], or becoming overwhelmed by the diagnosis, often seen in individuals and families with type 1 diabetes [T1D]); not comprehending the extent to which diabetes can be managed; the degree of personal responsibility required for management; and the perceived benefits and barriers to taking action. Professional support to address these reactions can be helpful in promoting self-management of diabetes.
Stigma Associated With Diabetes
- Weight-based stigma—the perception and experience of being discriminated against due to one’s body weight—can be perpetuated by providers in health-care settings. When present, this can lead to worsening distress, diminished quality of life, as well as decreased diabetes self-management behaviours. Health-care providers must be aware of their own biases and be able to communicate in a non-stigmatizing manner about weight-related issues and diabetes management.
Financial Burden of Diabetes
- Diabetes is an expensive illness to live with and to manage well. People living with diabetes should ask their health-care teams for help and health-care providers should recognize the key role they play in accessing financial supports. Advocacy and activism are helpful and often necessary to manage the cost of living with diabetes.
- The costs associated with diabetes can have effects on the physical and emotional well-being of people with diabetes.
Risks Associated With Diabetes and Psychiatric Conditions
- A wide range of psychiatric disorders (beyond the serious mental illnesses of major depressive disorder [MDD], bipolar and related disorders, and schizophrenia spectrum disorders) put people at higher risk for developing diabetes (usually T2D) compared to the general population.
- People living with diabetes and MDD are at increased risk for earlier all-cause mortality compared to people living with diabetes without a history of MDD.
- Compared to those with diabetes only, individuals with diabetes and mental health concerns are at risk for functional impairment, diabetes complications, and increased health-care costs, often coupled with decreased participation in diabetes self-care and decreased quality of life.
Diabetes in Pregnancy
- Individuals with diabetes in pregnancy are at an increased risk of developing mental health disorders (e.g. depressive and anxious symptoms) and psychological distress throughout the pregnancy. Receiving effective emotional and tangible support, in addition to medical advice, can help buffer these negative outcomes.
Risks for Children and Adolescents
- Youth with diabetes are at risk for having psychosocial symptoms and diabetes self-management difficulties. Regular assessments during routine diabetes care are especially helpful during adolescence and the transition to young adulthood.
- It is important to also assess the emotional functioning of the whole family/home environment—including parent/caregiver distress and fear of hypoglycemia—in order to understand the potential impact of these influences on younger people with diabetes.
Diabetes in Older Adults
- Depressive symptoms in older adults with T2D are an important risk factor for cognitive impairment and are associated with an increased risk of earlier mortality.
- Older people with T2D experience an increased disease burden and are more likely to have multimorbidity (an increased likelihood of complications and other adverse outcomes).
Substance Use and Diabetes
- Substance use is linked with multiplicative health risks and can be a factor in the development of new-onset T2D, as well as worsening health outcomes among those with established diabetes.
- Smoking cigarettes and/or alcohol consumption are risk factors for the development of T2D and adverse cardiovascular events in people with established diabetes.
- People prescribed insulin are more susceptible to the harmful effects of recreational substance consumption, particularly alcohol use.
- Screening for substance use followed by a brief intervention can be helpful, and approved pharmacotherapies for tobacco, alcohol, and opioid use disorders are safe for use in people with diabetes.
COVID-19
- People with diabetes are at higher risk for developing more severe complications from a COVID-19 infection. Preventative measures, such as keeping a safe distance from others, wearing a mask in public, regular handwashing, and keeping up to date on vaccinations, help reduce the risk of acquiring the virus and potentially the severity of the illness.
Screening and Assessment
- All individuals with diabetes, as well as the parents or caregivers of youth with diabetes, should be screened at appropriate intervals for the presence of diabetes distress, as well as symptoms of common psychiatric disorders.
- People with diabetes are at risk for developing a wide array of mental health conditions—especially mood and anxiety disorders—and should be screened regularly for symptoms that may be part of a psychiatric condition.
Psychosocial Treatment Approaches to Managing Diabetes
- Person-centred approaches using motivational interviewing, cognitive behaviour therapy (CBT), acceptance and commitment therapy, stress management, coping skills training, family therapy, and collaborative case management should be incorporated into primary care, wherever possible.
- Building self-management skills, employing educational interventions that facilitate adaptation to diabetes, and addressing co-occurring mental health issues that reduce diabetes-related distress, fear of hypoglycemia, and reluctance to initiate insulin when recommended, are all helpful.
Use of Psychotropic Medications
- There are effective treatments for the disabling symptoms that comprise psychiatric conditions. Regular use of medication can be a crucial element in helping people maximize their function and reduce symptom severity.
Monitoring Metabolic Risks
- Individuals taking psychiatric medications, particularly (but not limited to) atypical antipsychotics, benefit from regular screening of metabolic parameters to identify glucose dysregulation, dyslipidemia, and changes in weight (and possibly other anthropometric measures) throughout the course of the illness so that appropriate interventions can be instituted if necessary.
Key Messages for People With Diabetes
Living With Diabetes
- Living with diabetes can be burdensome and anxiety provoking. The constant demands of having to care for the illness take a psychological toll. As a result, many people struggle to accept the diagnosis or proposed treatment plan and delay actively participating in diabetes care, which only worsens the long-term outlook.
Psychological Reactions to the Diagnosis of Diabetes
- Diabetes is often associated with distress over the need for daily self-care, adding stress to relationships, a significant emotional burden. It is important to be compassionate with yourself and accept your emotions as valid responses to a chronic condition. In addition to self-care, seeking out support by talking to your friends, family, and members of your diabetes health-care team about how you are feeling can be helpful. Your team can help you to develop effective coping skills and direct you to mental health–care services that can make a difference for you.
Stigma Associated With Diabetes
- Diabetes-related or weight-related stigma (feeling or experiencing social judgement) is common and can lead to a decreased sense of well-being, as well as making you feel less motivated to care for your diabetes.
Financial Burden of Diabetes
- Caring for diabetes effectively can be expensive, and can exceed the ability of many people to manage financially. There may be ways to reduce these costs. So, if your finances are suffering, let your health-care team know—it is possible that something helpful can be done.
Risks Associated With Diabetes and Psychiatric Conditions
- Mood and anxiety symptoms are common in people with diabetes and can be impairing enough to lead to a formal psychiatric diagnosis. Eating, sleeping, and stress-related problems are also common. Speak to your health-care providers about the concerns that you have.
- Mental health issues can affect your ability to cope with and care for diabetes. Caring for your mental health is just as important as caring for your physical health and improves the long-term picture for your diabetes.
- People diagnosed with many psychiatric conditions appear to have a higher risk of developing diabetes than the general population.
Diabetes in Pregnancy
- If you have diabetes and are planning on becoming pregnant (or already are pregnant), your diabetes care team is available to offer psychosocial support and, if necessary, referrals to mental health resources.
Risks for Children and Adolescents
- Younger people often face psychological struggles that negatively impact managing diabetes. Share your physical and emotional struggles with your diabetes care team so they know what to help you with.
- Diabetes care impacts the whole family, so it is important to also discuss parent/caregiver’s psychosocial functioning with the diabetes team. There are interventions that can improve everyone’s well-being.
Diabetes in Older Adults
- Older individuals with T2D have more complications and adverse outcomes compared to younger individuals with T2D, which can make treatment more challenging and complicated.
Substance Use and Diabetes
- Smoking causes greater health harms in people with diabetes compared to those who do not have the illness. Even 1 cigarette per day is harmful to your health. If you smoke, consider asking for support from your health-care provider to help you quit. Using a smoking cessation medication (nicotine patches, varenicline, or bupropion) together with counselling more than doubles your chances of quitting successfully.
- If you currently do not drink alcohol, it is a healthier decision to not start. For people who drink alcohol, it is imperative to reduce intake to minimize adverse health outcomes. This may mean consuming a maximum of 2 standard drinks per week, which has been linked with causing the least potential for harm. Consuming over 4 standard drinks per occasion has the potential to negatively affect diabetes care. Ask your health-care provider for support if you wish to reduce your alcohol use.
- Substance use with cannabis, stimulants, or illicit opioids may interfere with your blood glucose levels and your ability to manage your diabetes, particularly if these substances are consumed on a regular basis or in a large quantity over a short time (binges).
COVID-19
-
Diabetes puts people at greater risk of having complications if you get infected with COVID-19. Preventative measures, such as keeping a safe distance from others, regular handwashing, and wearing a mask in public places, reduce the chance of acquiring COVID-19. Keeping up with vaccinations may reduce the severity of the infection if you do get it. You must do your best to reduce your chances of developing long COVID.
Screening and Assessment
-
Your health-care provider can offer screening questionnaires that you can complete to help better understand your experiences and aid in planning treatment for diabetes. There are questionnaires to screen for diabetes-related concerns, as well as for general psychological distress. Screening questionnaires can be completed prior to your appointment and the results discussed at your visit.
Psychosocial Treatment Approaches to Managing Diabetes
-
Diabetes care teams can help you manage the degree of distress that you are experiencing with strategies that are specific to living with diabetes. As well, they can arrange a referral to mental health services for concerns that may not be directly related to diabetes.
Use of Psychotropic Medications
-
Medications, when taken regularly, can make a significant contribution to your health and ability to live your life with fewer troubling symptoms. If a medication has been recommended, consider giving it a good trial (taking it long enough as prescribed to determine if it is working) and then reporting the results to your clinician. Hopefully, you can find medications that make a positive impact on your health and are tolerable (few or no side effects).
Monitoring Metabolic Risks
-
Your mental health medications may need to be monitored for possible side effects. Monitoring your glucose levels, lipid levels, blood pressure, and changes in weight will give you peace of mind that your major health risks are being covered.
Introduction
Diabetes mellitus is a disease that takes a heavy toll on the lives of people who have received the diagnosis. For those diagnosed with T1D, it is a major life stress (and can become a medical emergency) that often dominates the focus of individuals and their families. T2D can be (often for the first several years) asymptomatic or cause symptoms that are relatively easy to ignore. Yet, minor metabolic aberrations develop into larger ones that eventually can affect most major physiological systems and lead to characteristic end-stage complications that threaten life, limb, and vital functions. Diabetes mellitus can be a challenge for the people who have it, as well as the network of people who seek to offer support.
Irrespective of which type of diabetes an individual has, it can be a significant daily burden from which there is no relief. Research has shown that people who live with T1D must make an estimated 180 health-care decisions each day [1].
Managing blood glucose levels within a narrow range is a constant, complex balancing act, and what works well one day may not work the next. Many people who do not live with diabetes don’t understand the persistent challenges involved in managing it and, in fact, can sometimes make those who have diabetes feel blamed or shamed for having it. Despite the fact that diabetes is caused by numerous complex factors—not all of which are within an individual’s control—many Canadians (with and without diabetes) view a person’s own behaviour as the most important contributing factor to the increasing rate of T2D [2].
The mental and emotional burden of living with diabetes can seem overwhelming, but can be reduced when caregivers have a fuller appreciation of this stress. Research has shown an increasingly clear relationship between diabetes and a variety of psychological reactions. These include expectable reactions to being diagnosed with a chronic metabolic illness, which can progress to established psychological syndromes specific to the experience of living with diabetes, finally increasing in severity to diagnosable psychiatric disorders. Another important contributor to psychological burden with diabetes is the social burden stemming from the judgement and stigma that accompanies life with diabetes. The 2018 Diabetes 360 report found that 33% of people with diabetes are hesitant to disclose their diabetes to others and 15% have experienced some form of discrimination, often due to misconceptions about the cause of the illness [3].
The context for understanding mental health issues in those living with diabetes begins with the acknowledgement or reflection that life involves continual challenges requiring daily coping efforts that necessitate sufficient resources and support. A primary drive for individuals is to try to maximize a sense of pleasure, and to minimize pain and distress [4].
When it comes to chronic diseases, such as diabetes, a treatment maxim is that “no one wants to be unwell.” The diagnosis of diabetes confers burdens and challenges that drain resources from other pursuits. One way of understanding this is to examine the relationship between life experiences and emotions, specifically:
- The experience of threat → feelings of anxiety
- The experience of loss → feelings of sadness/depression
- The experience of unfairness → feelings of anger [5]
This perspective offers insight into the mental health issues that people living with diabetes might experience. Inquiring into experiences of threat (e.g. nocturnal hypoglycemia), loss (e.g. recalling the more carefree experience of not having diabetes), and unfairness (e.g. navigating eating in social circumstances) can help empathize with the burden associated with diabetes. Since diabetes self-management affects almost every aspect of daily living, the burden of management is high, since it falls on individuals and their supports [6,7].
Psychological Adaptation/Expectable Reactions to the Diagnosis of Diabetes
Diabetes is a demanding chronic disease for both individuals and their families [8]. It is not surprising that some individuals struggle with acceptance of the diagnosis. If no one wants to be unwell, embracing the illness and its treatment involves a willingness to tackle the behavioural, social, and emotional burdens associated with successful diabetes management. Disease acceptance issues might be more likely to occur during life transitions or illness transitions. Individuals diagnosed with diabetes may follow expectable reactions to receiving bad news (i.e. denial, anger, sadness, bargaining, shock, rationalization, etc.) and get stuck at any of these stages. In order to maximize one’s ability to reduce the potential harms from diabetes, individuals must accept the diagnosis and be willing to fully participate in recommended treatments.
Similarly, while we have access to many highly effective medical therapies and supporting technologies in diabetes management, persons with diabetes are the ones who must enact these strategies. Accordingly, attitudes and perspectives are critical to assess and address in any care plan. Treatment acceptance is an important issue that should not be overlooked in supporting individuals living with diabetes. Both disease acceptance and treatment acceptance can be understood through a validated assessment strategy called the Health Belief Model [9,10].
This model involves assessing perceptions of disease susceptibility, disease severity, benefits to action, barriers to action, self-efficacy, and cues to action. Asking questions about these areas and incorporating the person’s attitudes into the care plan is both recommended and consistent with contemporary views on person-centred care [11].
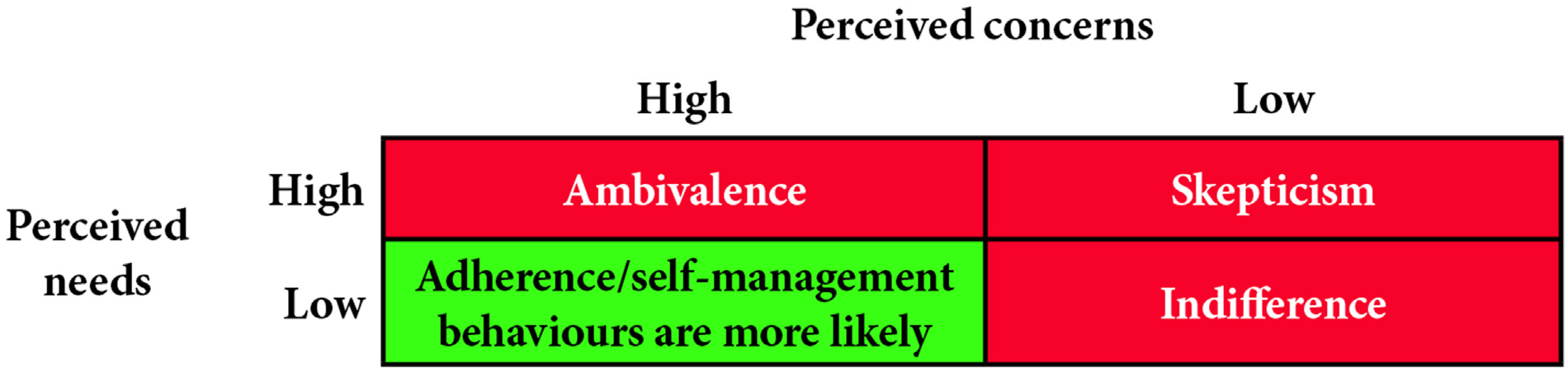
The Health Belief Model is also helpful in understanding the acceptance of medical treatments. Specifically, there is strong evidence supporting the needs and concerns analysis regarding any specific recommended medical treatment. Adherence to medical therapies is critical to diabetes outcomes and is often suboptimal, and the needs and concerns analysis can help providers identify reasons for this [12].
Providers are encouraged to ask persons with diabetes at the time of medication initiation/review about the degree to which they believe they need the medication, and the extent to which they have concerns about the medication. Use of the following matrix (Figure 1
Difficulties in accepting the diagnosis and treatment recommendations do not necessarily reflect a pathological process. These reactions are based on specific beliefs of the individual, such as someone on higher doses of medication must be in worse shape. Often clinicians are aware of the importance of psychological issues but feel ill-equipped to address them [13].
One way to support providers in addressing emotional issues is to separate the constructs of distress and psychopathology. Distress can be driven by diabetes-specific issues, problems of living, and/or psychopathology. Diabetes-specific distress should be considered to be within the scope of diabetes care providers to address, where problems arising from living-based distress or psychopathology-based distress (such as comorbid psychiatric disorders) are better managed in collaboration with mental health–care providers [14].
Established Psychological Syndromes Related to the Diagnosis of Diabetes
The significance of diabetes-specific psychosocial issues (and comorbid psychiatric disorders) is that they are associated with reduced participation in self-management activities, decreased quality of life, and poorer treatment outcomes that include diabetes complications and early mortality [15]. There are 3 established psychological conditions associated with the lived experience of diabetes that should be monitored and managed: diabetes distress, hesitance to initiate insulin when recommended, and fear of hypoglycemia (for those at risk).
Diabetes distress (DD) refers to the negative emotions and burden of self-management related to living with diabetes. This term is used to describe the despondency and emotional turmoil specifically related to living with diabetes, in particular, the need for continual monitoring and treatment, persistent concerns about complications, and the potential erosion of personal and professional relationships [16,17].
DD has received extensive research over the last decade. A PubMed search (performed August 5, 2022) of the title term “diabetes distress” yielded 532 publications, including 17 systematic reviews. Evidence is clear that DD is common, affecting approximately one-third (36%) of those with diabetes [18].
DD can be measured using validated scales, both for T1D [19] and T2D [17,20]. Additionally, the Problem Areas In Diabetes (PAID) scale has been validated for use with T1D and T2D [21].
DD is a critically important mental health issue to be aware of, and should be part of regular screening [22]. DD is associated with elevated A1C levels, higher diastolic blood pressure, and increased low-density lipoprotein cholesterol levels [23–25]. Furthermore, individuals with higher levels of DD were found to have a 1.8-fold higher early mortality rate, a 1.7-fold increased risk of cardiovascular disease [26], and a lower quality of life [27]. Risk factors for developing DD include being younger; being female; having a lower degree of education; living alone; having a higher body mass index (BMI); lower perceived self-efficacy; lower perceived provider support; poorer quality diet; greater perceived impact of glycemic excursions; and greater number of diabetes complications [28,29].
Hesitancy to initiate insulin when recommended (also called psychological insulin resistance [PIR] or insulin refusal [IR]) refers to a strong negative response from people with T2D to the recommendation from health-care providers that they would benefit from adding insulin to their regimen. This can be a common reaction, particularly for individuals with T2D who may have previously been successfully managed with oral antihyperglycemic agents. Individuals may hold beliefs that the need for insulin is a sign of personal failure in their self-management, or that their illness has become much more serious. Further, many people report fear or anxiety about having to self-administer injections, and have a low level of confidence in their ability to manage their blood glucose with insulin [30,31]. It is important for diabetes providers to be aware of PIR/IR because it is a major factor associated with diabetes treatment inertia [32].
Identifying the attitudes underlying this reluctance is an opportunity for diabetes providers to ask permission to educate about evidence versus perception. Common underlying beliefs are perception of worsening disease severity, the addition of insulin representing a personal failure, perceived loss of control, injection-related anxiety, anticipation of pain, low self-efficacy, and perceived lack of any positive gains [33].
If health-care providers can reframe the beliefs around initiating insulin, and relate it to the pathophysiology of diabetes, health outcomes can improve.
Fear of hypoglycemia (FoH), for those with the potential for hypoglycemia, is a common occurrence and a major behavioural and emotional burden. Hypoglycemic experiences, especially serious or nocturnal episodes, can be traumatic for both individuals and their family members. A common strategy to minimize FoH is compensatory hyperglycemia, where individuals either preventatively maintain a higher blood glucose level, or treat hypoglycemia in response to perceived somatic symptoms without objective confirmation by capillary blood glucose concentrations[34–37]. This process, if left unmanaged, can negatively impact glycemic target achievement, increase the risk of complications, and reduce quality of life.
Figure 1
Determining perceived concerns and needs when considering medications.
Summary of Psychological Syndromes Associated With Diabetes
Challenges accompanying the diagnosis of diabetes include adjustment to the illness, participation in the treatment regimen, and psychosocial difficulties at both a personal and an interpersonal level [38,39]. Stress, deficient social supports, and negative attitudes toward diabetes can impact on self-care and glycemic levels [40–44]. Diabetes management strategies ideally incorporate a means of addressing the psychosocial factors that impact individuals and their families. Both symptom measures (e.g. self-report measures of various symptoms) and methods to arrive at psychiatric diagnoses (e.g. structured interviews leading to Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision [DSM-5-TR] diagnoses) [45] have been developed. Given that people with diabetes are directly responsible for 95% of diabetes management [46], identifying significant psychological reactions in diabetes is important since depressive symptoms are a risk factor for difficulties with diabetes self-management [47-49] and outcomes, such as early mortality [50,51].
Distinguishing Diabetes Distress From Major Depressive Disorder
While DD, MDD, and the presence of depressive symptoms (that do not meet the threshold for the diagnosis of MDD) do share similar symptomatology, DD has been most shown to have the strongest effect in causing adverse diabetes outcomes [52–54]. Some of the distinguishing features between DD and MDD are summarized in Table 1
Stigma: Comorbid Diabetes and Mental Health Issues
Stigma—defined as the experience of perceived or direct social judgement (social stigma)—often results in discrimination or exclusion, including in health-care settings (structural stigma). The reported prevalence of social stigma among adolescents and young adults with T1D has been reported to range between 47%-65%. Stigma has been also associated with both hyper- and hypoglycemia, as well as reports of a reduced sense of well-being and self-efficacy for managing diabetes [57].
Diabetes-related stigma is often associated with visible diabetes management activities (e.g. use of technology, blood glucose checks, verbalized rationale for food choices), leading to coping by avoidance with regard to diabetes care [57].
Approximately half of adults with T2D report experiencing both general diabetes-related stigma, as well as stigma based on weight status [58].
Endorsement of higher degrees of weight-based stigma (i.e. being discriminated against or experiencing prejudice/differential treatment due to body weight) is associated with increased levels of diabetes-specific distress and weight-bias internalization (self-stigma) in adults with higher weight status and/or T2D [59].
Weight-based stigma may also occur in health-care settings and can negatively impact the quality of the patient-provider interactions [59], as well as health outcomes (i.e. risk of elevated cortisol levels, higher blood pressure, decreased glycemic stability) [60]. Health-care providers need to be aware of their own weight-stigma biases and language in their verbal and written communication [58,60].
Training in the use of motivational interviewing techniques to improve the quality of communication around weight-based discussions can be helpful [60,61].
| Table 1 Comparison of the main features and assessment methods: Diabetes distress vs major depressive disorder |
||
|---|---|---|
| Diabetes distress | Major depressive disorder | |
| Assessment instrument | Diabetes Distress Scale (DDS) T1D (28 items) DDS-T2D (17 items) DDS-T2D Revised: Core scale (8 items); Sources (21 items) |
Patient Health Questionnaire for Depression: PHQ-9 (9 items) [55, 56] |
| Format | Self-report using ratings from 1 to 6 based on feelings and experiences over the past week | Self-report using ratings from 0 to 3 based on feelings and experiences over the past 2 weeks |
| Features | DDS-T1D: Powerlessness, management distress, eating distress, negative social perceptions, physician distress, and family/friends distress DDS-T2D: Emotional burden, physician-related distress, regimen-related distress, interpersonal distress DDS-T2D Revised: Management demands, long-term health concerns, hypoglycemia concerns, health-care access concerns, shame/stigma concerns, health-care provider concerns, and interpersonal demands concerns |
Vegetative symptoms, such as sleep, appetite, and energy level changes Emotional symptoms, such as low mood and reduced enjoyment of usual activities Behavioural symptoms, such as agitation or slowing of movements Cognitive symptoms, such as poor memory or reduced concentration or feelings of guilt; thoughts of self-harm |
Financial Burden/Financial Distress of Diabetes
Diabetes is a chronic condition associated with significant direct costs (e.g. medications, diabetes supplies, travel to physician and allied health-care provider appointments, food plans recommended for diabetes, etc.), as well as significant indirect costs (e.g. decreased productivity, management of diabetes complications, hospitalizations related to diabetes, etc.). It has been found that treatment participation in diabetes care is affected by these direct and indirect costs [62,63].
People affected by diabetes tend to have lower incomes than the general population. Depending on location, age, household income, medications, and medical devices used, people with T1D in Canada may face an annual out-of-pocket expense of up to $18,306 for costs associated with use of insulin pumps and continuous glucose monitoring devices. The average out-of-pocket cost associated with managing T1D may be as high as 20% of the total household income. In the case of people with T2D in Canada, the annual out-of-pocket cost can be as high as $10,014 and can account for up to 16% of the total household income. When there are multiple members of a household living with diabetes, the impact will be even greater. Depending on the location of the individual in Canada, there can be significant inequality in the share of these costs being covered by provincial/territorial governments, ranging from 0% to up to 100%. For people with T2D, government plans cover <20% of the costs for almost half the provinces and territories in Canada. The Kirby/Keon Senate Study and the Romanow Royal Commission on the Future of Health Care defined the threshold for catastrophic drug costs as 3% of gross income. This threshold was exceeded in 57% of T1D and 45% of T2D representative provincial and territorial scenarios in a recent update by Diabetes Canada, which suggests that these individuals are highly likely to be non-concordant with their prescriber’s recommendations.
Similar to these Canadian statistics, data from other countries also illustrate how financial burden can affect the capacity of a person to manage their diabetes. For instance, people taking insulin (a direct cost) report cost-related underuse of this treatment, and are more likely to have higher glycemic levels as a result [64].
A recent study suggested that young adults with T1D who report increased financial burden of diabetes are far less likely to achieve glycemic targets compared to those that do not report financial burden of diabetes. Cost concerns were described as all-consuming and a source of fear and feelings of isolation. Diabetes cost concerns intensified feelings of limitation and unfairness [65].
A US database study showed that people taking insulin with higher levels of treatment participation/self-management had significantly lower adjusted all-cause total costs than people with lower levels of adherence/self-management. This is despite the fact that the direct drug costs were much higher in the adherent group [66].
Multiple studies have established that the increased costs of diabetes therapy are associated with inadequate adherence, which eventually affects outcomes. Given the deleterious effects of cost-related underuse of therapy and the eventual complications of suboptimally controlled diabetes, it is imperative that health-care providers regularly ask about the affordability of therapy [67].
The 2021 National Health Interview Survey by the Centers for Disease Control and Prevention found that about 16.5% of people with T1D and T2D who use insulin rationed its use. The most common forms of insulin rationing included delaying purchase (all insulin users), followed by taking less than required (T1D more so than T2D) [68].
Members of diabetes care teams should inquire about the financial burden the illness is causing and help with access to fiscal supports available through government and other community programs (where applicable and available).
Figure 2
Framework for understanding the intersection of mental health and diabetes.
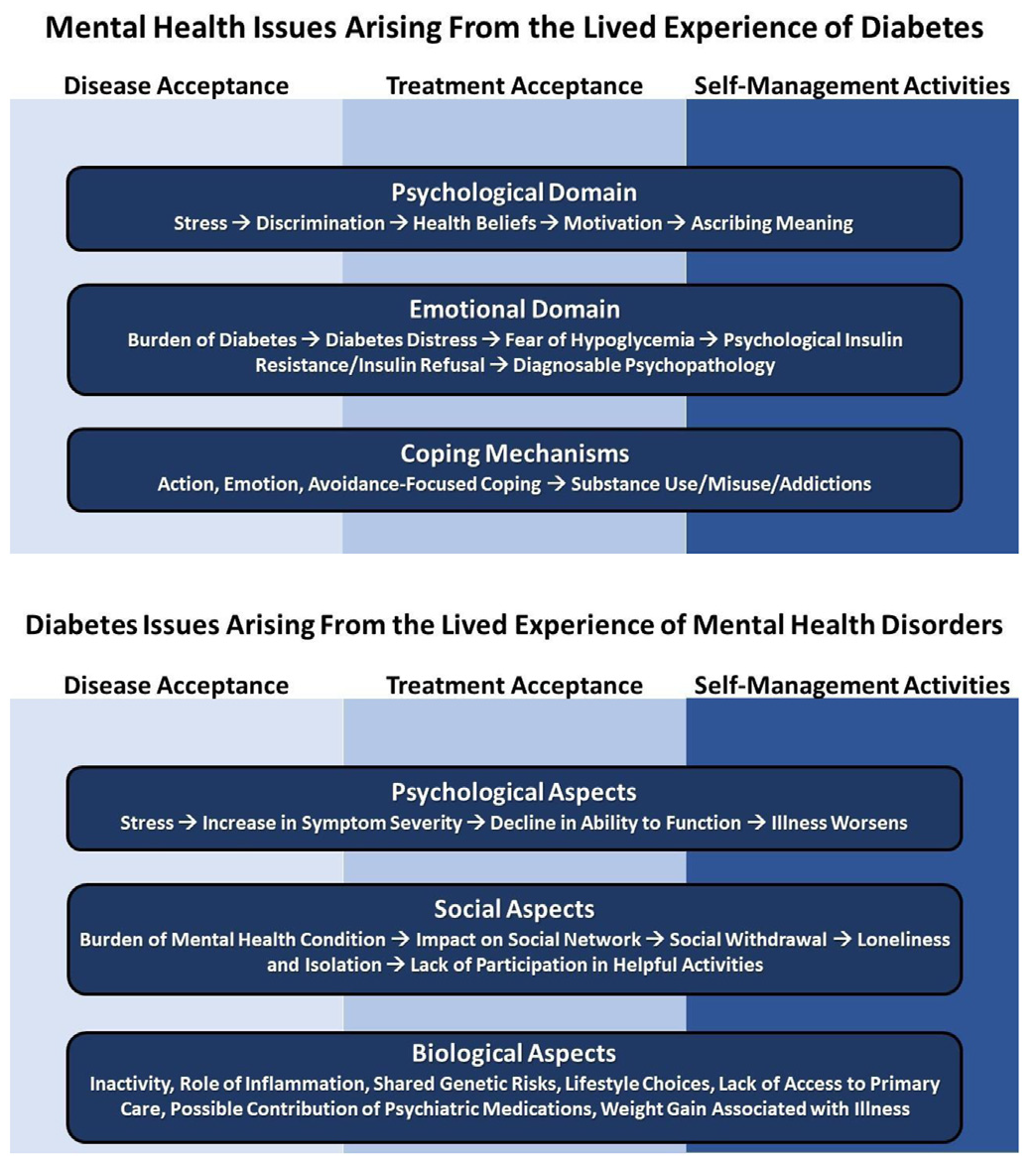
Figure 3
Psychiatric conditions that increase the risk of developing diabetes.
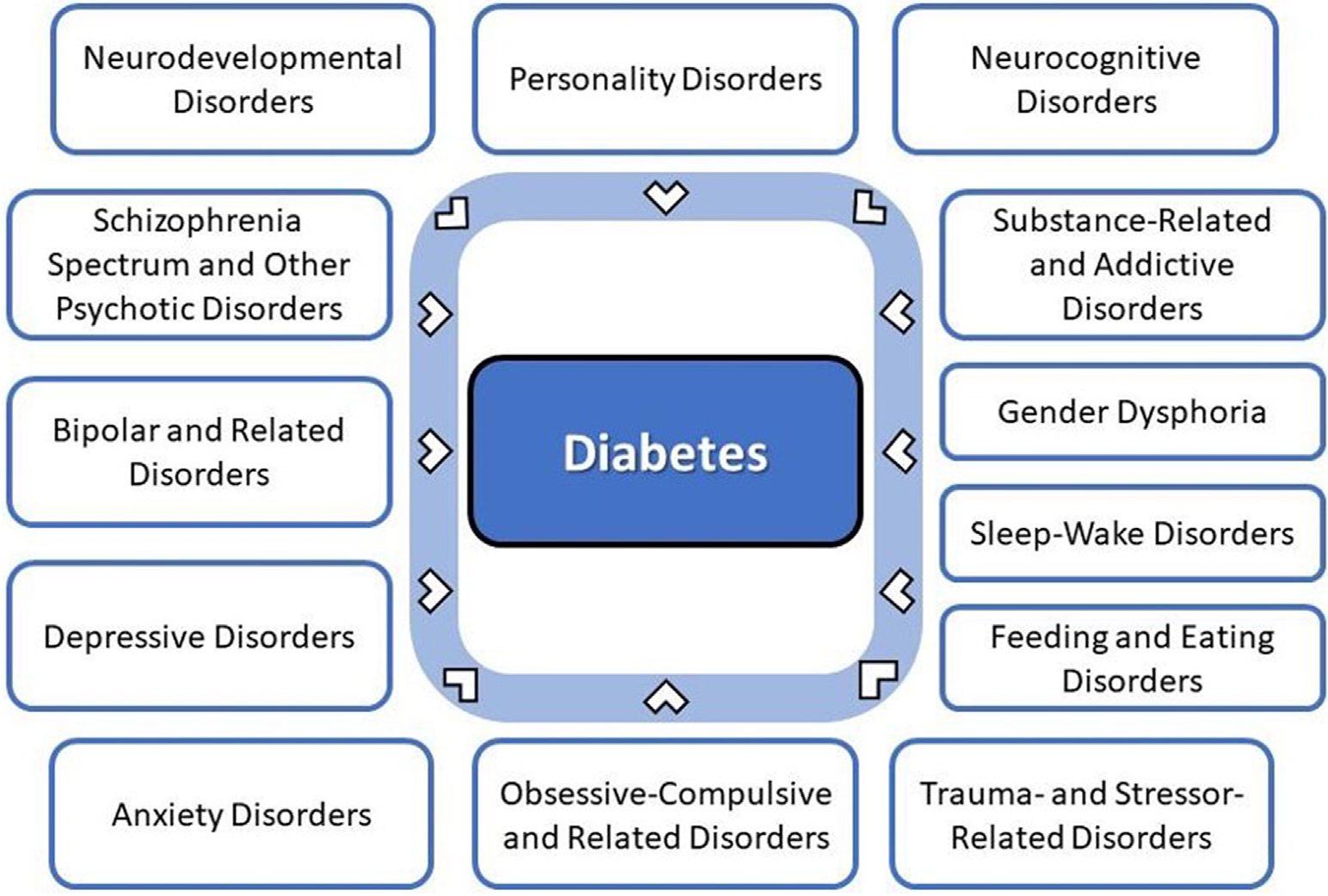
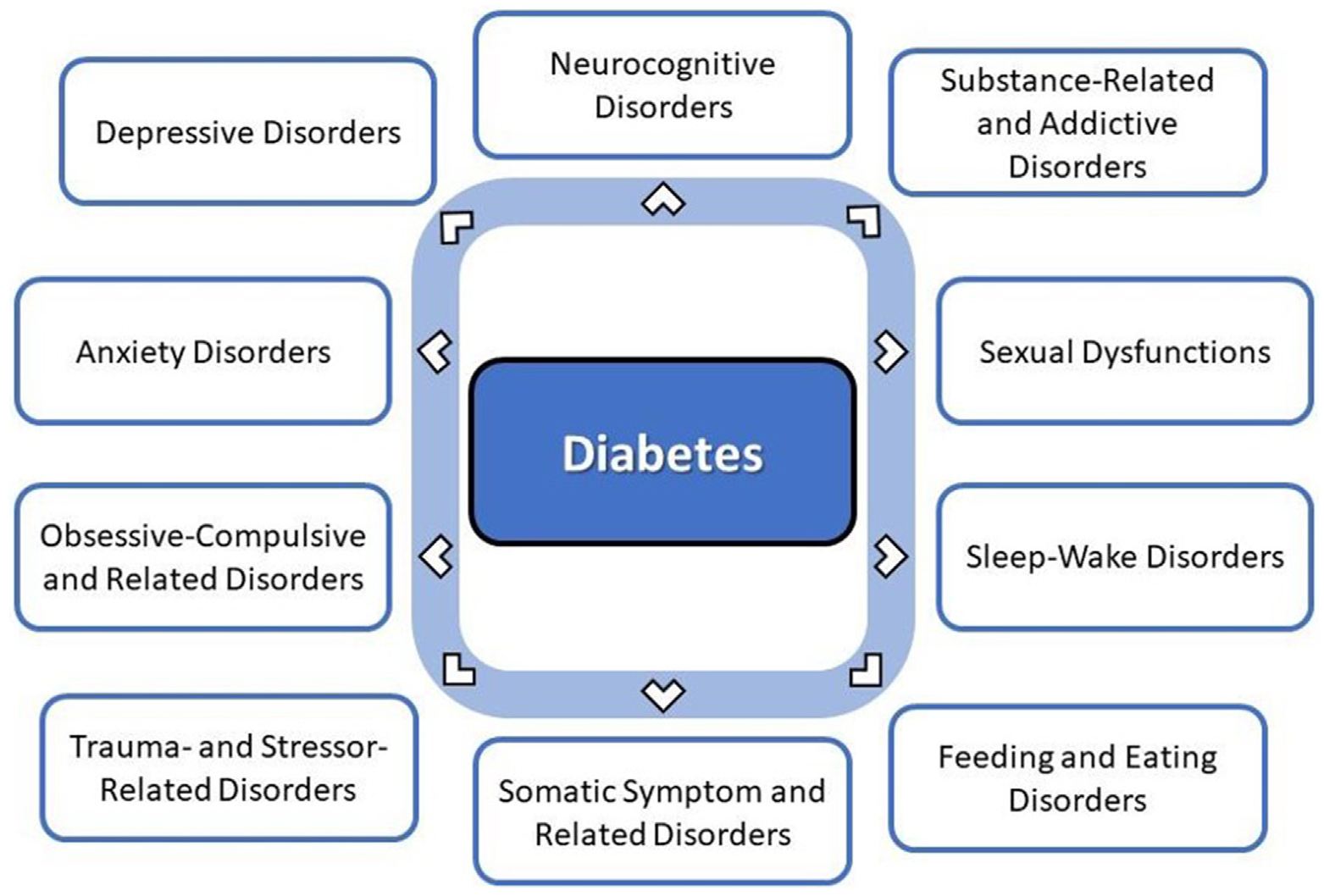
Figure 4
Diabetes increasing the risk of developing select psychiatric disorders.
Psychiatric Conditions in Adults
Individuals with serious mental illnesses—particularly those with depressive symptoms—and people with diabetes share reciprocal susceptibility and a high degree of comorbidity (Figures 3
The interplay between psychiatric disorders and diabetes is illustrated in Figure 4. The psychiatric disorders listed here principally (but not exclusively) contribute to the risk of developing T2D.
Neurodevelopmental disorders
People with intellectual disability or autism spectrum disorder were found to have a 1.6- to 3.4-fold higher age-adjusted odds of having obesity, as well as developing T1D or T2D compared to those without these conditions [72,73].
However, other studies have not established this risk, so these findings should be considered speculative [74].
The prevalence rate of T1D in people with Down's syndrome can be up to 10.6%, which is considerably higher than the general population [75].
A population-based data study in Taiwan found children (average age 8.6 years) diagnosed with attention-deficit/hyperactivity disorder (ADHD) had higher prevalence of T2D than people without ADHD (0.9% vs 0.4%, p<0.001). After adjusting for age, sex, index year, geographic location, and body weight, ADHD was significantly associated with a prior diagnosis of T2D (OR=2.75, 95% confidence interval [CI]=1.82–4.16). However, no significant association was observed between ADHD and T1D [76].
Schizophrenia spectrum disorders
A robust finding across many studies is that the prevalence of T2D in people with schizophrenia and schizoaffective disorder is 2- to 3-fold higher than in the general population [77–81].
Schizophrenia and other psychotic disorders may contribute an independent risk factor for diabetes. People diagnosed with psychotic disorders were reported to have had insulin resistance/glucose intolerance prior to the development of antipsychotic medication [82–84]. The Clinical Antipsychotic Trials for Intervention Effectiveness (CATIE) study found that of the individuals with schizophrenia who participated in the study, 11% had already been diagnosed with diabetes (T1D and T2D combined) [69]. The prevalence of metabolic syndrome was approximately twice that of the general population [85]. Diabetes and schizophrenia together lead to more cardiovascular complications and all-cause mortality compared to people with diabetes alone [86]. Whether the increased prevalence of diabetes is due to the effect of the illness (such as advanced glycation end products), antipsychotic medications, or other factors, individuals with psychotic disorders represent a particularly vulnerable population [87].
Furthermore, repeated relapses in schizophrenia leads to a higher risk of developing diabetes than does the first episode of psychosis. Women also are at higher risk of developing diabetes. Diabetes generally develops 1 to 2 decades after the onset of symptoms in serious mental illnesses, such as schizophrenia [88–92].
Bipolar disorders
The dominant finding from studies suggests that the prevalence of T2D in people with bipolar disorder is 2 to 3 times higher than in the general population [81–84[, along with at least double the risk of metabolic syndrome [14,93].
One study demonstrated that over half of people with bipolar disorder were found to have impaired glucose metabolism, which was found to worsen key aspects of the course of the mood disorder[94]. In this same study, impaired glucose tolerance (IGT) was found to be an associative factor (and possibly the precipitating step) in the development of bipolar disorder [94]. While insulin resistance or IGT does not cause bipolar disorder, the associated inflammation may unmask bipolar disorder in people predisposed to developing it. Insulin resistance is associated with a less favourable course of bipolar illness, more cycling between mood states, and a poorer response to lithium [95].
Significant work has gone into unravelling the role of inflammation as an important etiologic factor in mood disorders (more so for bipolar disorder than for MDD) [96].
Depressive disorders
The prevalence of clinically impactful depressive disorders among people with diabetes is approximately 30% [97–99]. The prevalence of MDD is approximately 10% [100,101], which is double the overall prevalence in the general population. The risk of developing MDD increases the longer a person has diabetes [102]. Clinically identified diabetes was associated with a doubling of the number of prescriptions for antidepressants. People with undiagnosed diabetes were not given an increase in prescriptions for antidepressants. This strengthens the hypothesis that the relationship between diabetes and depression may be attributable to factors related to diabetes management [103]. Individuals with MDD have approximately a 40% to 60% increased risk of developing T2D [103-105]. The prognosis for comorbid MDD and diabetes is worse than when each illness occurs separately [106]. MDD in people with diabetes amplifies symptom burden by a factor of about 4 [107]. Episodes of depression in individuals with diabetes are likely to last longer and have a higher chance of recurrence compared to those without diabetes [108]. Episodes of severe hypoglycemia have been correlated with the severity of depressive symptoms [109,110]. MDD has been found to be underdiagnosed in people with diabetes [111].
Studies examining differential rates for the prevalence of depression in T1D vs T2D have yielded inconsistent results [97,112]. One study found that the requirement for insulin was the factor associated with the highest rate of MDD, regardless of the type of diabetes involved [113]. Treatment with metformin may enhance recovery from MDD in T2D [114].
Risk factors for developing MDD in individuals with diabetes are as follows [115–119]:
- Female sex
- Adolescents/young adults and older adults
- Lower socioeconomic status
- Few social supports
- Stressful life events
- Glycemic instability, particularly recurrent hypoglycemia
- Higher illness burden
- Longer duration of diabetes
- Presence of long-term complications
Intensive lifestyle intervention designed to induce weight loss by providing intensive group and individual support for people with T2D with overweight or obesity reduced the risk of depressive symptoms by 15% [120].
Risk factors (with possible mechanisms) for developing diabetes in people with depression are as follows:
- Physical inactivity [121], having overweight, obesity [120], which leads to insulin resistance
- Psychological stress leading to chronic hypothalamic-pituitary-adrenal dysregulation and hyperactivity stimulating cortisol release, also leading to insulin resistance [122–127]
- Hippocampal atrophy and decreased neurogenesis [128]
Some of the mechanisms underlying this association are thought to be autonomic and neurohormonal dysregulation, hippocampal structural changes, inflammatory processes, and oxidative stress [128].
Comorbid MDD worsens clinical outcomes in diabetes, possibly because the accompanying lethargy lowers the energy available for self-care, resulting in lowered physical and psychological fitness, higher use of health-care services, and reduced participation in medication regimens [129,130]. MDD is also associated with increased cardiovascular mortality [131–133]. Treating depressive symptoms more reliably improves mood than it does glycemic stability [134–137].
MDD increases the risk of all-cause hospitalizations for persons treated for diabetes. This increased risk is independent of medication self-management difficulties, or other potential factors [138]. Inadequate social support increases the risk of MDD in people with T2D [139].
There does not appear to be a significant association between the severity of depressive symptomatology and higher A1C levels. However, increased depressive symptomatology was associated with higher A1C values among participants with fewer social supports [140].
Anxiety disorders
Anxiety is commonly comorbid with depressive symptoms [141]. One study estimated that 14% of individuals with diabetes experienced generalized anxiety disorder (GAD), with double this figure experiencing a subclinical anxiety disorder, and triple this figure having at least some anxiety symptoms [142]. Anxiety disorders were present as comorbid conditions in one-third of people with serious mental illnesses and T2D, and were associated with increased depressive symptoms and decreased level of function [143]. A 21-year follow-up study in Australian women suggests that long-term anxiety has been associated with an increased risk of developing T2D across the reproductive span [144].
Alternately, in an epidemiological study with 10-year follow-up, no significant relationship was found between anxiety and development of diabetes-related complications among those with prevalent T2D. This large study showed that anxiety disorders were not associated with a greater risk of developing T2D or the risk of diabetes complications in people already diagnosed with diabetes [145].
A multicentre international study spanning 15 countries looked at people aged 18 to 65 years with T2D treated in outpatient settings who were administered the Mini-International Neuropsychiatric Interview. The study found that female gender, the presence of diabetes complications, longer duration of diabetes, and more glycemic instability were significantly associated with comorbid anxiety disorders [146].
Obsessive-compulsive and related disorders
Individuals with obsessive-compulsive disorder (OCD) have an increased risk of T2D compared with the general population (adjusted hazard ratio = 1.22; 95% CI 1.13–1.31). Compared to people with OCD who do not take serotonin reuptake inhibitors, those taking higher doses of these medications and who had a longer duration of treatment demonstrated significantly diminished risks of metabolic and cardiovascular complications, irrespective of whether they were also taking antipsychotic medications [147].
Stress, trauma, abuse, and neglect
A history of significant psychological adversity or trauma—particularly early in life—increases the risk for developing obesity, diabetes, and cardiovascular disease [148]. Higher BMI, leptin, blood pressure, fibrinogen, and decreased insulin sensitivity have been found in people with significant trauma histories [149]. Post-traumatic stress disorder (PTSD) was found to cause a 40% increased risk of developing T2D, while those with subsyndromal traumatic stress symptoms had a 20% increased risk [150].
Traumatic symptoms may increase the risk for developing diabetes and other cardiovascular illness through reduced physical activity, poorer diet, greater likelihood of tobacco consumption, escalating BMI, and MDD [140].
There is a significant association between psychological trauma and higher A1C values. Adequate social support can attenuate the association between psychological trauma and A1C values [151].
Dissociative identity disorder
No conclusive evidence could be found at the time of writing regarding an association between dissociative identity disorder and diabetes, apart from a case report about hyperglycemia-associated dissociative fugue (organic dissociative disorder) in an older male [152].
Somatic symptom disorders
Non-specific premonitory symptoms can be prodromal signs of illnesses well before actual onset, and this includes T2D [153].
Somatic symptoms prior to the onset of T2D are chiefly related to hyperglycemic states and acute metabolic disturbances, with key symptoms being polyuria, polydipsia, weight loss (sometimes along with polyphagia), and blurred vision. People reporting these symptoms are at increased risk of developing T2D [154].
Feeding and eating disorders
Anorexia nervosa, bulimia nervosa, and binge eating disorder (BED) have been found to be more common in individuals with diabetes (both T1D and T2D) than in the general population [155]. Eating disorders are common and persistent, particularly in females with T1D [156,157]. Elevated BMI is a risk factor for developing both T2D and MDD [158].
Depressive symptoms (not severe enough to be MDD) are highly comorbid with eating disorders, affecting up to 50% of individuals with eating disorders [159].
Night eating syndrome (NES) is characterized by the consumption of >25% of daily caloric intake after the evening meal and waking at night to eat, on average, at least 3 times per week. NES has been noted to occur in individuals with T2D and depressive symptoms. NES can result in weight changes, poor glycemic management, and an increased number of diabetes complications [160].
Up to 20% of people with T2D have an underlying eating disorder, the most common being BED. The prevalence of BED in people with T2D can be up to 25%, which is significantly higher than the 2%-3.5% prevalence seen in the general population.
T1D with disordered eating (T1DE)—often called diabulimia—is an eating disorder that only is seen in people with T1D when they decrease or stop taking their insulin in an attempt to lose weight. Although diabulimia is not a formal diagnosis, it has garnered significant exposure in the media that medical and psychiatric communities acknowledge the term. Offering psychological support is the mainstay of treatment for people with diabulimia. Clinicians should consider each individual’s concerns about weight or physical appearance, challenges in adjusting to diabetes, past traumatic experiences, and the value of supportive relationships in order to deliver effective psychological treatment [161-163].
Elimination disorders
People with diabetes commonly experience problems with bladder and bowel control. However, no conclusive evidence is presently available to support a more formal association between elimination disorders and diabetes.
Sleep–wake disorders
The risk of developing T2D is associated with alterations in sleep pattern, including <6 h and >9 h total sleep time, initial insomnia, sleep maintenance problems, obstructive sleep apnea (OSA), and erratic sleep. The elevated risk is comparable to traditional risk factors for T2D, such as having excess weight, having a positive family history, and physical inactivity. Pooled relative risks (RRs) of total sleep time are:
- ≤5 h total sleep time → RR 1.48 (95% CI 1.25–1.76)
- 6 h total sleep time → RR 1.18 (95% CI 1.10–1.26)
- ≥9 h total sleep time → RR 1.36 (95% CI 1.12–1.65)
Poor sleep quality, OSA, and shift work were associated with greater risk of developing T2D, with a pooled RR of 1.40 (95% CI 1.21–1.63), 2.02 (95% CI 1.57–2.61), and 1.40 (95% CI 1.18–1.66), respectively. In comparison, the pooled RRs of living with overweight, having a family history of diabetes, and being physically inactive were 2.99 (95% CI 2.42–3.72), 2.33 (95% CI 1.79–2.79), and 1.20 (95% CI 1.11–1.32), respectively [164].
Sexual disorders
Both T1D and T2D are established risk factors for sexual dysfunction in men [165-168].
There is a 3-fold greater risk of erectile dysfunction (ED) in men with diabetes compared to those who do not have it, likely due to vascular causes [165,169].
Men with diabetes have a lifetime ED prevalence of between 35% and 75% [170].
Women with either T1D or T2D have been found in some studies to have an increased prevalence of sexual dysfunction compared to women without diabetes [167,171,172].
Female sexual dysfunction appears to be more likely due to secondary social and psychological impacts of diabetes rather than the direct physiological consequences [167,172,173].
There is no robust evidence available at this time showing that other sexual or paraphilic disorders have an association with diabetes [174].
Gender dysphoria
An increased prevalence of T1D in transgender children and adults has been described (up to 9.5 times in one study) [175].
However, the correlation of T1D with gender dysphoria appears to exist equally for all transgender populations [176,177].
Various factors may explain the increasing prevalence of T1D in transgender populations, including psychological stress. Clinicians should attempt to look for environmental triggers, such as psychological minority stress (defined as the relationship between minority and dominant values and resultant conflict with the social environment experienced by minority group members) experienced by young people with gender dysphoria. Such sources of stress may affect the pathogenesis and management of T1D. Better clinical outcomes may result with early detection and adequate support.
A Dutch case-control study found an increased prevalence of T2D among transgender populations when compared to both age-matched, non-transgender males and females, though this study did not adjust for other risk factors [177,178].
In a study of the effects of administering gender-affirming hormones on insulin sensitivity in transgender populations, transgender women (those receiving estrogens or anti-androgens) evidenced a reduction in markers of insulin sensitivity; there was no change in transgender men (those receiving androgenic medications) [179].
People with established diabetes undergoing gender-affirming surgeries constitute a special group for whom efforts to effectively manage glucose levels is desirable. Genital surgeries and breast/chest surgeries involve microvascular techniques, and healing, avoidance of infection, functionality, and cosmetic enhancement all have better outcomes with optimization of glycemic stability. Although the diagnosis of diabetes in itself may not be a contraindication for any of these procedures, interprofessional coordination between the surgical team and the clinicians managing the diabetes is advisable [180].
At present, there appears to be no significant relationship between receiving gender-affirming hormone therapy and diabetes risk, or impact on established diabetes. Accordingly, no specific recommendations can be put forth at this time for diabetes screening in transgender populations, regardless of hormone administration status.
Impulse-control disorders
In a study of 50,000 people using data from 19 countries, the authors identified 2,580 cases of adult-onset diabetes diagnosed in individuals aged 21 years and older. After factoring for the presence of comorbid MDD, this study found that, among impulse-control disorders, only intermittent explosive disorder appeared to be an independent risk for diabetes (OR 1.6; 95% CI 1.1–2.1) [181].
People whose weight is in the obese range but who do not have T2D have been found to have somewhat more rigid behaviours along with more compulsive personality traits compared to people with both obesity and T2D, who may demonstrate more impulsivity with their decisions, which may negatively influence diabetes self-management [182].
Substance use disorders
The exact prevalence of substance use disorders among individuals with diabetes is difficult to establish, and the presence of substance use disorders may contribute to unique challenges in this population. Recreational substance abuse is associated with increased rates of hospitalization and readmissions for diabetic ketoacidosis (DKA) [183]. Furthermore, substance abuse and psychosis among individuals with T1D and T2D increases the risk of all-cause mortality [184–186].
Neurocognitive impairment/disorders
T2D is a recognized risk factor for the development of various subtypes of dementia and mild cognitive impairment [187].
MDD is an important risk factor in the development of cognitive impairment in people with T2D, the risk being 2.5 times compared to people with diabetes without MDD. Although certain inflammatory markers, such as C-reactive protein and interleukin 6 (IL-6), are associated with MDD, there is presently no clear link supporting the hypothesis that systemic inflammation mediates the relationship between MDD and dementia [188].
Personality traits/disorders
Personality traits or disorders that put people in constant conflict with others or engender hostility have been found to increase the risk of developing T2D [189]. People with chronic, significantly negative mood states and social inhibition were less likely to follow a healthy diet or to consult health-care professionals when problems developed with their diabetes management. They report more barriers surrounding medication use, diabetes-specific social anxiety, loneliness, and symptoms of depression and anxiety [190].
A population-based, matched cohort study in Denmark found an increased risk of personality disorders (unspecified) in only girls with a diagnosis of T1D. An Australian study confirmed an overall increase in the risk of personality disorders of more than 2-fold following T1D onset, but did not differentiate between sexes [191].
In T2D, impaired personality functioning, as manifested by greater difficulties in personal relationships, mood dysregulation, impulse-control problems, and problems with interpersonal communication were correlated with deterioration in plasma glucose levels during the first 6 months of a standardized disease management program. However, the degree of depressive symptoms did not show this correlation [192].
Neuroticism—the disposition to experience negative emotions—including anger, anxiety, self-consciousness, irritability, emotional instability, and depression is associated with decreased T2D risk, even after controlling for ethnicity, age, depressive symptoms, and BMI.
Type A behaviour is characterized by a constant sense of time pressure, a strong appetite for competition, and the achievement of goals. Extraversion and Type A behaviours do not appear to be significant risk factors for T2D [193–195].
A descriptive cross-sectional study examined 294 participants (104 with T1D and 190 controls). People with high levels of resiliency estimated their degree of diabetes management inaccurately by reporting a high degree of perceived adherence, which was not in keeping with their more objective A1C levels (suggesting overconfidence). With respect to psychological health factors, people who demonstrate more resilience appear to have better overall adjustment, demonstrating fewer emotional problems in managing T1D.
People exhibiting controlling traits (sometimes referred to as “overcontrolled”) with A1C levels indicative of adequate metabolic management in T1D, however, were found to have the most accurate adherence estimation. Factoring in people’s personality styles can help predict participation in self-care recommendations (overcontrolled personalities) and whether their estimation of successful diabetes management is likely to be accurate [196].
Psychiatric Disorders and Adverse Outcomes
Two independent systematic reviews with meta-analyses showed that MDD significantly increases the risk of all-cause mortality among individuals with diabetes compared to those with diabetes without MDD [197,198]. Older adults with diabetes and MDD may be at particular risk [184]. Individuals with bipolar disorder, schizophrenia, or other psychotic disorders, and who have comorbid diabetes, are at increased risk of rehospitalization following medical-surgical admissions [199].
A large prospective cohort study determined that the presence of MDD in people with both T1D and T2D is associated with greater risk of developing chronic kidney disease compared to people without MDD [200].
Comorbid MDD or anxiety are associated with significantly longer hospital length of stay, as well as for adolescents with T1D hospitalized for DKA [201].
A meta-analysis of 11 cross-sectional and prospective cohort studies showed that MDD is significantly associated with higher incidence of diabetic retinopathy in individuals with T2D. However, it is unclear if this is a causal association [202].
Impact on length of hospital stay
Two studies reported an increase in length of stay of close to 4 days in individuals with diabetes and a comorbid mental illness [203,204].
Individuals with T2D are more likely to have a longer length of stay in inpatient mental health settings compared to people with T1D. Those with T2D are likely to have more comorbid conditions, increasing illness severity and necessitating longer hospital stays. More resources are likely to be needed to ensure a safe and seamless hospital discharge. The needs of people with T2D may be different than those with T1D, but it is unclear if the difference in pathophysiology alone accounts for differences in length of stay [205].
Considerations in Pregnancy
Gestational diabetes mellitus
A recent systematic review of the associations between gestational diabetes mellitus (GDM), anxiety, and depression in pregnant individuals found a bidirectional relationship in that anxiety and depression (as well as other stressors, such as a history of childhood sexual abuse and experiencing intimate partner violence) during pregnancy resulted in a higher incidence of GDM [206]. Additionally, a diagnosis of GDM increased the subsequent incidence of anxiety and depressive disorders [207].
Another meta-analysis indicated that the highest levels of depressive symptoms for individuals with GDM occur right around the time the condition is diagnosed [208]. This may be due to the increased psychological strain of having a new diagnosis that could negatively impact pregnancy outcomes and the increased demands in diabetes self-management tasks [207].
However, a population-based study in Canada explored mental illness rates (including anxiety and MDD) in individuals prior to pregnancy, during pregnancy, and postpartum. It was found that, although the prevalence of mental health issues was higher in those with GDM versus those without GDM, there appeared not to be a temporal relationship between GDM and subsequent incidence of psychiatric diagnoses [209]. Differences were hypothesized to be more likely related to gestational increases in weight [210]. Additionally, there did not appear to be significant mental health differences in those diagnosed with GDM early in pregnancy versus during the typical screening period for GDM in pregnancy [211].
Despite these disparate findings, the consensus is that there is a higher prevalence of psychiatric symptomatology in individuals with GDM and that the symptoms are often underdiagnosed [212].
Optimized pregnancy outcomes can be seen with:
- Increased health-care provider awareness of the potential impact on mental health at diagnosis of GDM
- Regular screening throughout the pregnancy and postpartum period (e.g. potentially at each prenatal visit following the GDM diagnosis)
- Routine referrals for mental health interventions (both traditional therapy and other options)
- Culturally sensitive measures [213–215]
Screening instruments and rating scales, such as the single-item Self-Rated Mental Health Question (SRMHQ), can be helpful in individuals with GDM [216]. A study using mindfulness-based counselling interventions has demonstrated some initial effectiveness in decreasing anxiety in individuals with GDM, but more research is needed to compare this treatment with other evidence-based approaches [217], as well as examine whether lifestyle-based interventions that address weight fluctuations during pregnancy are effective at reducing depression symptoms [218].
Pregestational/pre-pregnancy diabetes
For those individuals with pregestational/pre-pregnancy diabetes (PGM), such as premorbid diagnosis of T1D or T2D, a Canadian-based population study found that there was a modestly higher incidence rate of mental health disorders (including MDD and GAD) in the pregnancy and postpartum periods than for those without PGM [219]. Another study examined the trajectory of depressive and anxious symptoms in a group of individuals with PGM only, and the results indicated that these symptoms remained unchanged from early to late pregnancy [220]. Optimal support for this population would involve:
- Early mental health screening, peer support options, and timely referrals for mental health treatment both during pregnancy and during the postpartum period
- Proactive psychosocial strategies from health-care providers on managing mood and anxiety symptoms prior to potential conception, as well as any individual with PGM during the perinatal period for all individuals with diabetes (regardless of pregnancy status) [221]
- Medical support beyond primarily focussing on reducing the risk of pregnancy complications (e.g. preterm delivery) [222]
Diabetes in pregnancy
GDM, PGM, and postpartum depression: A population-based study examining postpartum depression (PPD) rates in individuals with diabetes in pregnancy (DIP), which includes individuals with either GDM or PGM, found a 1.5-fold increased risk for those with a history of MDD prior to pregnancy [223]. Another recent meta-analysis replicated the association between those with DIP and PPD but cautioned that when those with GDM versus PGM were compared, the individuals with GDM were the ones more at risk for developing PPD [224]. Another study found that although individuals with DIP all had significant levels of distress, the highest level of negative pregnancy outcomes was found in those with PGM and negative psychological outcomes were found in individuals with GDM [225].
Clinically significant DD (upwards of 58% in one study) can be present even if no diagnosable psychiatric conditions were found in individuals with DIP [212].
The SARS-CoV-2 (COVID-19) pandemic can also worsen symptoms. One study of individuals with DIP found that both anxiety and depression severity were high (approximately 80% and 60%, respectively), which is higher than reported prevalence rates in pregnant individuals without diabetes during COVID-19 [226]. In addition, 2 factors (unintended pregnancies and lower social support) were associated with higher levels of anxious and depressive symptoms for individuals with DIP. This may also be related to the effects of social isolation during the pandemic based on fears of a more severe COVID-19 infection for those with diabetes [226], which may improve with diabetes education and medical support that focuses on the emotional burden of DIP and diabetes regimen-related concerns [227].
Optimal care for people with GDM and PGM would involve:
- Screening practices that include an assessment of one’s history of MDD or significant depressive symptoms prior to pregnancy in addition to current mental health functioning
- Targeted diabetes education and tailored medical treatment plans for the different populations of pregnant individuals with GDM and PGM, which may have differing psychological trajectories [225,228]
Individuals with pregnancy in diabetes have a higher prevalence of various psychiatric conditions (particularly mood and anxiety disorders), which are often underdiagnosed [212]. One study found that higher levels of medical support experienced by individuals with DIP significantly reduced levels of anxious and depressive symptoms and may buffer the negative outcomes [229].
Children and Adolescents
T1D in children and adolescents
For children and adolescents, there is a need to identify mental health disorders and psychosocial issues associated with T1D in order to be able to institute early interventions. Children and adolescents with T1D have significant risks for mental health issues, including depressive symptoms, anxious symptoms, altered feeding and eating, and disruptive behaviours [230–232]. These risks increase significantly during adolescence [233,234] and into young adulthood. Studies have shown that mental health disorders predict difficulties with diabetes management and glycemic variability [235–238] and worsen medical outcomes [47,239–241]. The more glycemic levels are not within target range, the probability of mental health issues also increases [242]. Adolescents with T1D have been shown to have rates of DD that are comparable to adults with T1D [16].
The presence of psychosocial symptoms and diabetes self-management issues in children and adolescents with T1D are often strongly affected by caregiver/family distress. It has been demonstrated that while parental/caregiver psychological issues are often related to psychological adjustment issues and glycemic variability [243–249], they also can negatively impact perceptions of the child's ability to manage diabetes [250].
An initial study of parental self-report suggests that the use of hybrid closed-loop systems for insulin delivery in children may help ameliorate some parental FoH and poor sleep quality symptoms that may lead to improved glycemic stability for the child [251]. Maternal anxiety and depressive symptoms are often associated with higher glucose instability and school absenteeism in younger adolescents with T1D, and a reduction in positive mood and motivation for their own diabetes care in older teens [252,253].
Eating disorders in pediatric diabetes
Ten percent of adolescent females with T1D meet DSM-5-TR criteria for eating disorders [45], compared to 4% of their age-matched peers without diabetes [254]. Eating disorders are also associated with less metabolic stability, in addition to an earlier onset and faster progression of microvascular complications [157]. Adolescent and young adult females with T1D who have difficulty achieving and maintaining glycemic targets—particularly if insulin omission is suspected—may also have problematic eating behaviours (including subclinical disordered eating behaviours and eating disorders).
Individuals with disordered eating behaviours may require different management strategies to optimize glycemic stability and prevent microvascular complications [254]. T1D in adolescent females appears to be a risk factor for development of a formal eating disorder, both in terms of an increased prevalence of established eating disorder features, as well as purposeful weight control through diabetes-specific means, such as insulin omission or restriction (often called “diabulimia”), significant carbohydrate restriction, and disinhibited eating when experiencing symptoms of hypoglycemia [255,256].
Other considerations in children and adolescents with T1D
The prevalence of anxiety disorders in children and adolescents with T1D in one study was found to be 15.5%, and mood disorders was 3.5%, with one-third having a lifetime prevalence of at least one psychiatric condition [257]. Another study of children with early onset (<5 years) of T1D and a diabetes duration of at least 10 years found elevated GAD symptoms in about 10% of the adolescent population, which was associated with both diminished general and diabetes-specific functioning [258]. The presence of psychiatric disorders was related to elevated glycemic levels and a lowered health-related quality of life score in a general pediatric quality of life inventory study [257]. In the diabetes mellitus–specific pediatric quality of life inventory, children with mental health disorders revealed more symptoms of diabetes, higher treatment barriers, and lower self-management behaviours than children without mental health disorders [257]. Adolescents with T1D ranked school as their number 1 stressor, their social lives as number 2, and having diabetes as number 3 [259].
Prevention and intervention in children and adolescents with T1D
Children and adolescents with T1D, as well as their families, benefit from screening for mental health disorders and psychosocial issues (also referred to as person-reported outcome measures [PROMs]) at the time of diagnosis, as well as at regular intervals [260]. Given the prevalence and impact of mental health issues, psychosocial screening of children and adolescents with T1D is just as important as screening for microvascular complications [261,262].
A promising addition to traditional in-person clinic visits is the use of telehealth services, which increased out of necessity during the COVID-19 pandemic but may be a lasting option. Online meeting rooms, such as virtual group appointments or digital health interventions (e.g. mHealth apps) demonstrate improvements in diabetes-related distress [263] and self-efficacy [264], as well as parental ratings of quality of life [265]. In order to prepare for the transition from pediatric to adult diabetes care, a transition plan should be initiated at around 12 years of age so that services (including diabetes education, transition readiness assessments, setting transition goals, etc.) can occur early enough to prepare adolescents and their families [266,267].
Psychological interventions, which include cognitive-behavioural as well as other complementary psychotherapy approaches (e.g. art therapy), have a positive impact on mental health of children and adolescents with T1D and their families [268, 269], including overall well-being [270], perceived quality of life [271,272], and reduction in depressive symptoms [269,273]. Psychosocial interventions can positively affect glycemic stability[274,275]. Other studies have demonstrated that psychological interventions can increase both diabetes self-management behaviours and frequency of in-target glycemic levels, as well as overall psychosocial functioning [276,277].
T2D in children and adolescents
Mental health concerns play a significant role in children and adolescents with T2D across all ethnic groups, particularly depression [278] and binge eating behaviours [279].
These psychosocial issues, along with disruptive sleep habits [280], are associated with lower diabetes self-management success and quality of life [231,281].
Rates of reported depressive symptoms ranged from 15%-36% in youth with T2D and have been found to be highest among females and youth with fewer social support as well as a family history of T2D [282]. Moderate-to-severe depression rates in young adults who were diagnosed with T2D in childhood have also been associated with high levels of DD [283].
Presently, there is a lack of high-quality research data on the impact of MDD and depressive symptoms in youth with T2D. The majority of the studies in this population do not assess for a formal diagnosis of MDD, although depressive symptoms are common in youth and more likely to be associated with adverse diabetes outcomes [282].
Considerations for Older People With Diabetes
T2D does not appear to be more common in geriatric-aged people with psychiatric conditions than similarly aged controls. The risk of developing a dementing illness in people is increased in those who have MDD (hazard ratio [HR] 1.83), T2D (HR 1.20), or both (HR 2.17) [284]. The presence of depressive symptoms in older adults with T2D is associated with increased mortality risk [285].
Older individuals experience a greater disease burden due to diabetes and are more likely to have multimorbidity and experience the adverse outcomes, including severe complications like diabetic neuropathy, nephropathy, retinopathy, or vasculopathy, which are seen in up to 20% of older people with T2D [286].
Totalling the PHQ-9 scores for the symptoms of diminished interest, sleep changes (increase or decrease), psychomotor changes (retardation or agitation), and diminished concentration symptoms to 4 or above has an enhanced specificity for detecting MDD in older people [287].
Overweight status, limited physical capabilities, and reduced activity level, along with the presence of more than 2 comorbid illnesses, were risk factors for MDD in older people with diabetes mellitus. In a case–control study done in China, metformin was found to reduce the risk of developing MDD in older people with diabetes [288].
Access to ongoing psychosocial interventions through technological platforms may potentially minimize diabetes complications and improve health-related outcomes [289,290]. Telehealth-related technologies can be effective in improving the clinical, behavioural, and psychosocial outcomes in people with diabetes above 50 years of age.
Prescription choices for older people with diabetes mellitus and MDD should factor in antidepressants with a higher likelihood of safety and tolerability [291].
Recreational Substance Use
Recreational substance use is common in Canada. Among the general population, the prevalence of consumption is: [292,293]
- 15% for problematic alcohol consumption
- 11% for daily tobacco
- 4.3% for daily cannabis
- 3% for opioid use for recreational/non-medical purposes
- 2% for cocaine use
- 0.2% for methamphetamine use
Most studies find that prevalence of substance use among people with diabetes mirror the prevalence rates found in people without diabetes. Excess substance use leads to physical health complications in major organ systems leading to increased morbidity and premature mortality. This makes substance use among people with diabetes of particular concern because of the additive health risks.
Evidence suggests that substance use has a complex effect on diabetes. In people without diabetes, consumption of tobacco or alcohol increases the risk of developing diabetes [294,295]. In persons living with diabetes, substance use is linked with adverse health outcomes, particularly complications of diabetes [296,297]. These observations can be partly explained by the deleterious effects of the substance directly on glucose homeostasis. There are indirect effects of substance use on one’s capacity to perform health-maintaining behaviours that are needed for prevention and self-management of diabetes [298].
Substance use and risk for developing diabetes
A large body of literature suggests that substance use is associated with greater risk for the development of T2D [294,295]. However, there is no evidence at present to suggest that substance use plays a role in the development of T1D, as many cases appear in childhood/adolescence prior to substance exposure.
Tobacco
A meta-analysis of 25 cohort studies found an increase in the relative risk for new-onset diabetes among people who smoke cigarettes (RR 1.44, 95% CI 1.31–1.58). The potential risk appears to be dose-dependent, with smokers using ≥20 cigarettes per day showing the highest risks [294].
The heightened risk for heavier smokers has a number of hypotheses, including the stimulant effects of nicotine leading to insulin resistance, the potentially toxic effects of substances (e.g. heavy metals found in tobacco) on the pancreas, and the positive correlation between the number of daily cigarettes smoked and abdominal obesity [299].
Quitting smoking, while having a myriad of health benefits, paradoxically appears to be associated with a transient increase in the risk of new-onset diabetes. In the first 2-6 years after quitting, the hazard ratio for new-onset diabetes in successful quitters is higher than with active smokers (HR 1.22; 95% CI 1.12–1.32). The risk is higher in people who gain weight after quitting smoking, with those who gain the most weight (>10 kg) having the highest risk. This risk peaks 5-7 years after quitting and declines over time [300]. The modest elevation in risk for new onset of diabetes after quitting does not negate the benefits of quitting smoking on cardiovascular health, as evidenced by a decrease in the incidence of acute coronary events and death [300].
Alcohol
On a cross-sectional level, the lowest risk for new-onset diabetes appears to be among those with moderate alcohol consumption. People who consume about 1 standard drink per day (10-14 grams of alcohol) showed an 18% reduction in relative risk compared to abstainers. The relationship was curvilinear, with highest risks observed in those with alcohol consumption over 4.5 standard drinks per day and people who abstain [295].
Events such as acute pancreatitis that follow heavier episodes of alcohol consumption are an established risk factor for new-onset diabetes [301].
Some studies suggest that the type of alcohol consumed may also influence the health benefits, with wine conferring greater risk reduction benefits than beer or spirits [302]. In the absence of high-quality literature linking alcohol consumption to reduced risk of diabetes, most scholars suggest that the purported benefit from alcohol consumption, if any, may be modest at best and conclusions from observational studies may have been exaggerated or biased by methodological factors such as the inclusion of people who quit alcohol due to health reasons being included in the abstainers’ group (often referred to as “sick abstainers”) [295].
Other substances
Compared with tobacco and alcohol, there is less evidence regarding the association of cannabis use and new-onset T2D. Two cross-sectional studies actually detected a modest reduction in the prevalence of obesity and diabetes among people who use cannabis [303,304], while 2 cohort studies reported conflicting results; one showing an increase in risk for pre-diabetes among those who consume cannabis that was not observed in the other [305,306].
Limited evidence exists regarding the risk of T2D in people who use opioids for non-medical purposes. Prescription opioids do not appear to be associated with an increase in the risk of new-onset diabetes [307].
Nevertheless, people with opioid use disorders who receive opioid agonist therapy (OAT) with methadone appear to be at a higher risk for developing diabetes compared with those receiving naloxone-buprenorphine [308].
Adverse effects of substance use on diabetes-associated comorbidities and complications
It is well-established that regular, sustained substance use is associated with unfavourable health outcomes. Among persons with diabetes, those with heavy substance consumption patterns exhibit higher rates of diabetes-related morbidity and earlier mortality [309]. The deleterious effects of substance use vary with age and type of diabetes. In people <30 years, most of whom have T1D, complications such as DKA and hypoglycemic events have been observed to be more common in those who consume substances [296,297]. In older people >30 years with T2D, micro- and macrovascular complications are associated more commonly with substance use [310,311]. The propensity of substances to worsen glycemic stability has been attributed to a direct effect on glucose homeostasis and an indirect effect mediated through diminished levels of diabetes self-management [298].
T1D
Cigarette smoking can interfere with glucose homeostasis among persons with T1D. Smoking is linked with greater odds of hypoglycemic events (OR 2.4; 95% CI 1.30–4.40) and greater variability in blood glucose levels [312].
Compared with non-smokers, smokers spent greater time in either hypoglycemic or hyperglycemic states and less in normoglycemia [313].
Hypoglycemia could be partly explained by a co-consumption of cigarettes and alcohol [314] and by inadequate diabetes self-management found among smokers [315].
In persons with T1D, alcohol reduces plasma glucose levels and interferes with hypoglycemic counter-regulatory mechanisms. The onset of hypoglycemia usually appears 6-8 hours following alcohol consumption. The sedating effect of alcohol may also reduce the awareness of hypoglycemia. Together, these effects of alcohol can increase the risk of severe hypoglycemic events [296].
Alcohol use among people with T1D can interfere with disease self-management and lead to missed doses of insulin [297], which may explain the greater risk of DKA among young people with T1D who misuse alcohol [183,316].
Managing alcohol consumption can be a challenge for young people in an environment that promotes alcohol use, such as post-secondary institutions [317].
Stimulants (e.g. cocaine, methamphetamine) are linked with hyperglycemic events though their stimulation of sympathetic transmission. Elevated catecholamine levels counter the effects of insulin, and, in combination with missed doses of insulin, can lead to DKA [318].
There is limited evidence available currently in the way of studies regarding the effect of cannabis use on people with T1D. Cannabis can interfere with glucose homeostasis indirectly via its appetite-promoting tendencies, and directly by an effect on gastrointestinal motility that can lead to vomiting. Cannabis may also interfere with self-management routines [319].
A recent study using the T1D Exchange Clinic Registry found that adults with T1D who reported moderate cannabis consumption had 2.5-fold greater risk for DKA [320].
Frequent events of hypoglycemia, hyperglycemia, and/or DKA that are related to substance use take a substantial toll on the health of young people with T1D. This group was associated with a 4-fold earlier mortality rate compared to the general population [321], with substance use being identified as a significant contributor [322,323].
T2D
A recent meta-analysis of longitudinal observational studies confirmed the deleterious effects of smoking on the health of people with diabetes. Compared with people who have never smoked tobacco, smoking had greater relative risks for early mortality (RR 1.55; 95% CI 1.46–1.64), coronary heart disease (RR 1.51; 95% CI 1.41–1.62), stroke (RR 1.54; 95% CI 1.41–1.69), and peripheral artery disease (RR 2.15; 95% CI 1.62–2.85) [310].
People who had quit smoking showed lower levels of risk for cardiovascular events and death compared with active smokers, but still had higher rates compared with lifetime non-smokers [310].
Data analysis by gender suggests that women who smoke have a greater risk for cardiovascular events and death compared with men. However, men and women appear to benefit equally from quitting [324].
The elevated risk for cardiovascular events and death associated with smoking can be attributed to its direct effect on insulin resistance, leading to worsening of glycemic levels as well as the propensity for atherosclerosis [325]. It is also suggested that smoking is associated with more difficulties in diabetes self-management practices [326].
The health effects associated with alcohol drinking among people with diabetes may follow a curvilinear relationship [311]. People who drink 1 standard drink per day appear to have the lowest risk for cardiovascular events, even lower than people who abstain. People consuming over 2 drinks per day have an associated greater risk than abstainers. The associated cardiovascular risk increases linearly with every drink beyond 2 drinks per day [327].
Similar to the association with the risk of developing T2D, scholars have questioned whether moderate alcohol consumption (1 standard drink per day) has a true protective cardiovascular effect or that the results are biased by inclusion of “sick abstainers” in the non-drinking group [328].
Alcohol is thought to be particularly detrimental to health when consumed in higher quantities. People diagnosed with alcohol use disorder experience worse outcomes compared to those without this condition. This includes higher odds ratio for myocardial infarction (OR 1.62; 95% CI 1.06–2.47) and cerebrovascular accident (OR 1.35; 95% CI 0.92–1.98) [309]. Heavy drinking is also linked with negative diabetes outcomes, such as increased odds for diabetic neuropathy (OR 1.27; 95% CI 1.10–1.46) (27%) [309].
Similar to smoking, the effects of alcohol consumption in higher quantities appear greater among women relative to men with diabetes in terms of mortality [327,329].
Engaging in heavier alcohol consumption appears to be particularly detrimental to the health of individuals treated with insulin, who are associated with a 6- to 10-fold greater risk for alcohol-related mortality compared with groups without diabetes matched for alcohol consumption [329].
Beyond the direct effect on glucose homeostasis, alcohol use was also found to predict lower adherence with diabetes self-management behaviours [298].
There is limited evidence that alcohol use disorder may interfere with participation in structured self-management diabetes education programs [330].
Information regarding the effect of other substances such as opioids, cannabis, and stimulants on diabetes-related complications is limited at this time. However, one study found a greater odds ratio for early mortality in people with diabetes who use cocaine (OR 1.61; 95% CI 1.21–2.14) and illicit opioids (OR 1.35; 95% CI 1.02–1.8) [309].
A study examining US Medicaid records found a greater rate of opioid prescriptions among people with diabetes compared to those without (61% vs 31%) [331], which may be related to conditions such as diabetic neuropathy. Dealing with comorbid chronic pain may distract both providers and people with diabetes from focusing on the management of diabetes [332]. This may partially explain why the use of prescribed opioids has been linked with poorer quality of diabetes care, including reduced lipid and glucose monitoring [333].
There is limited evidence of the effect of long-term OAT on persons with diabetes. Stabilization of the opioid use disorder may improve the capacity for diabetes self-management and explain the improvements in A1C seen with buprenorphine/naloxone treatment [334].
Considerations for reducing harm from substance use
Tobacco
Systemic screening for and documentation of smoking status is widely endorsed in most health-care settings, and smoking cessation is promoted as a key activity for people with diabetes (i.e. ABCDESSS: A1C, blood pressure, cholesterol, drugs, exercise, self-management/screening/stopping smoking) [241].
Individuals who smoke tobacco should be offered support for quitting. Brief interventions for smoking (even lasting just 2-10 minutes) include psychoeducation on the benefits of quitting, assessing the level of interest in making a quit attempt, and responding appropriately with treatment or referral for treatment (5As: Ask, Advise, Assess, Assist, Arrange).
For those not ready to quit, a brief intervention can help individuals identify the relevance of quitting to support favourable diabetes and health outcomes. Elucidation of the existing barriers and identification of opportunities for change can be achieved by discussing the 5Rs of smoking: Relevance, Risk, Reward, Roadblocks, Repetition. Brief interventions, such as the 5As and 5Rs, increase the odds of quitting successfully [336].
The resources for brief tobacco interventions are made available by the World Health Organization (https://apps.who.int/iris/bitstream/handle/10665/112835/9789241506953_eng.pdf).
People with T1D and T2D have similar success rates to populations without diabetes when using approved treatment for smoking cessation. Quitting success is enhanced when individuals attempt to quit with approved pharmacotherapy (e.g. nicotine replacement therapy, varenicline, bupropion, etc.) combined with behavioural counselling [337,338].
| Table 2 Recreational substance use and the effects on diabetes |
|||
|---|---|---|---|
| Recreational substance |
Risk for developing diabetes | Health effects in people with T1D | Health effects in people with T2D |
| Tobacco cigarettes | Increased [300] | Greater glucose variability Hypoglycemia |
Coronary heart disease Stroke Peripheral artery disease [310] |
| Alcohol | Increased when drinking over 4 drinks per day [295] | Hypoglycemia Reduced hypoglycemia awareness [296] |
Hypoglycemia Reduced hypoglycemia awareness in people treated with insulin or sulphonylurea Cardiovascular risk increases linearly with every drink beyond 2 drinks per day Mortality risk increases when heavy drinking occurs in people treated with insulin [329] |
| Cannabis | Equivocal [305,306] | DKA [320] | Not available |
| Opioids | Not available | Not available | Not available |
| Stimulants | Not available | Hyperglycemia DKA [318] |
Increased risk of earlier mortality [309] |
Alcohol screening and brief interventions
Systematic screening for alcohol use in health-care settings can increase identification and timely treatment of alcohol misuse. The most common screening tool for alcohol is the Alcohol Use Disorders Identification Test (AUDIT-C). AUDIT-C screens for the frequency and intensity of alcohol consumption [339].
Scores range from 0-12 and a positive screen is 3 or 4 and above for women and men, respectively. Those with positive screens should be offered a brief intervention for alcohol reduction, which consists of psychoeducation on the risks of excess drinking and the benefits of reducing/quitting for health delivered in a patient-centred manner using a motivational interviewing approach [340].
These brief interventions are called SBIRT (screening, brief intervention, and referral for treatment), and have been shown to be effective for both the general population and people with T1D and T2D [340,341].
Recently, SBIRT has been delivered through the internet and found to be effective in reducing alcohol consumption among college students with T1D [342].
Persons who are unable to make changes to their alcohol use on their own should be offered a referral to specialized addiction treatment. Treatment consisting of addiction counselling and anti-craving pharmacotherapy is the mainstay of care for people with an alcohol use disorder. Approved anti-craving pharmacotherapy (e.g. naltrexone, acamprosate, or disulfiram) increase the success of addiction psychosocial counselling and are safe for use in people with diabetes.
The recent 2022 Canadian Low-Risk Alcohol Drinking Guidelines: Final Report from the Canadian Centre on Substance Use and Addiction (CCSA) urges Canadians to “rethink the way we drink” and reduce alcohol consumption to limits lower than those published in their 2018 guidelines. The lowest risk for health-related harm was seen in people who consume 2 or less standard drinks per week [343].
Alcohol consumption at a level of 3-6 standard drinks per week is associated with increased risk for cancer, and 7 drinks per week or more increases cardiovascular risk [310,344].
Cannabis
Legalization of cannabis in Canada in 2018 led to an increase in use amongst all age groups, but young people in particular. Legalization was followed by a position paper in 2019 from Diabetes Canada [345]. For persons with diabetes who choose to use recreational cannabis, potential harm can be reduced by following recommendations made by Canada’s Lower-Risk Cannabis Use Guidelines [346]. These recommendations include avoiding cannabis use during adolescence, avoiding high-potency THC products (i.e. concentrates) and synthetic cannabis (e.g. “spice”), avoiding smoking cannabis to protect lung health, and avoiding daily/regular use. Following these recommendations may also reduce diabetes-related adverse effects that have been associated with cannabis, such as poor diabetes self-management, glycemic instability, and DKA [345].
Individuals who are unable to decrease their cannabis use on their own should be offered a referral to specialized addictions treatment. To date, there are no approved medications for the treatment of cannabis use disorder, and addiction counselling is considered the mainstay of care [347].
Most recently, there is some evidence to suggest that glucagon-like peptide-1 (GLP-1) receptor agonists may play a beneficial role in the treatment of a number of substance use disorders, including tobacco and alcohol. Since this class of medications is currently approved for use in people with T2D, it may be helpful in the treatment of persons with co-existing T2D and substance use disorders [348], however, conclusive evidence is lacking at this point in time.
Suicide
A review article found that people with both T1D and T2D had increased rates of suicidal thoughts, suicide attempts, and completed suicide compared to the general population [349].
T1D
A systematic review and meta-analysis of more than 50 studies reported that individuals with T1D have a risk of completed suicide 2.25 times that of those without T1D [350].
T2D
People with newly diagnosed T2D had a rate of suicide attempts of almost 10%, which is twice the rate estimated in the general population. The rate of past suicide attempts in individuals with diabetes and comorbid depression was reported at over 20% [351].
Adolescents and young adults
A study of Canadian adolescents and adults reported that individuals with T1D had a higher lifetime prevalence of suicidal ideation (15.0%) as compared with people without T1D (9.4%) [352].
A thorough literature review with practical recommendations for providers (e.g. staff training, screening implementation, brief interventions, prevention efforts, and education and support tools) for reducing suicide risk in youth and young adults with T1D is available [353].
COVID-19 and Mental Health
Acute infections
The COVID-19 pandemic involved the institution of unprecedented public health measures, depleted an already overburdened health-care system, and set off highly polarizing misinformation wars. Among the plethora of other physical and psychological symptoms and the impact on lifestyle-related behaviours, COVID-19 appears to be a causative factor in the development of both T1D and T2D [354]. A meta-analysis reviewing over 3,700 individuals found a pooled proportion of 14.4% for newly diagnosed diabetes in people recently hospitalized with COVID-19 infections [355]. The CoviDiab Registry (covidiab.e-dendrite.com) is a project developed by researchers and clinicians to record features of new-onset, COVID-19–related diabetes as well as severe metabolic disturbances in pre-existing diabetes (i.e. DKA, hyperosmolarity, severe insulin resistance).
A bidirectional relationship appears to exist between COVID-19 infections and diabetes [356].
A United States Department of Veterans Affairs study of over 180,000 participants with no prior diagnosis of diabetes and who tested positive for COVID-19 found that beyond the first 30 days of infection, survivors demonstrated increased risks and burdens for diabetes, and an increased use of antihyperglycemic agents [357].
Pre-morbid diabetes is also associated with an increased risk of COVID-19 complications. Outcomes for people who had COVID-19 and diabetes but were without other comorbidities found an increase in severe complications, including pneumonia, excessive uncontrolled inflammation, a hypercoagulable state, and escalated glucose metabolism dysregulation. The authors concluded that diabetes was a risk factor that would lead to rapid progression of symptoms and more severe negative health outcomes of COVID-19 infections [358].
Long COVID
Post-infection syndromes are common with other viruses, such as Epstein-Barr, cytomegalovirus, West Nile, and enteroviruses, and we must now add COVID-19 to the list. Debilitating symptoms that persist well past the acute phase of a COVID-19 infection have been reported with increasing frequency in the general population [359].
COVID-19 infections can be divided into 3 phases: acute (lasting up to 4 weeks), sub-acute (lasting between 4 and 12 weeks), and chronic (starting after 12 weeks). It is known by a variety of names, including post-acute COVID-19 syndrome (PACS), post-COVID condition, post-acute sequelae (PASC) of COVID-19, and—an emerging favourite—long COVID, with those who experience it identifying themselves as “COVID long-haulers” [360].
While there is currently no standardized definition of long COVID, it can be at least conceptualized as the lack of a return to pre-infection state of health by 4-12 weeks (depending on the definition used). It appears to be triggered by a reaction to the virus that either does not resolve or causes new symptoms to appear after the acute phase of exposure to the virus.
Lacking formalized criteria for the diagnosis, pathognomonic symptoms, or definitive laboratory findings, long COVID involves a prolonged recovery that includes persistent physical and psychological symptoms. Long COVID has no set pattern to the development of symptoms and a variable course. Those who experience it can have difficulty convincing others of their struggles with serious and persistent symptoms.
The risk of developing long COVID involves only an exposure to the virus and has not yet been found to be related to the severity of the acute infection (except for an intensive care unit admission, which is a predictive factor on its own). End-organ damage in the acute phase and pre-existing illnesses (especially respiratory) appear to increase the risk. Other factors found to increase risk are advanced age, high BMI, and certain ethnicities [361].
In the general population, females outnumber males by about 3 to 1 in experiencing long COVID symptoms. Being unvaccinated appears to approximately double the risk of developing long COVID as well [362,363].
The most commonly reported symptoms of long COVID are dyspnea, fatigue, cognitive impairment, and anxious and depressive symptoms, which can significantly impair the ability of individuals who also have diabetes to participate fully in diabetes self-management behaviours [364,365].
In summary, diabetes is associated with an increased risk of COVID-19 complications [357]. COVID-19 vaccinations reduce the risk of developing long COVID [362]. The symptoms of long COVID significantly reduce an individual’s ability to manage diabetes [359] and overlap with prominent symptoms in MDD and GAD [366].
Screening and Assessment of Mental Health in Diabetes
Mental health symptoms
Because of the prevalence of DD and psychiatric comorbidity, and the negative impact that these factors have on glycemic management, early morbidity, and quality of life, it is recommended that individuals with diabetes be regularly screened with validated questionnaires or clinical interviews. The available data do not currently support the superiority of any particular depression screening tool [367]. Currently available screening instruments have a sensitivity of between 80% and 90% and a specificity of 70% to 85% [367]. Scales that are in the public domain are available at www.outcometracker.org/scales_library.php. Patient Health Questionnaire (PHQ-9) screeners are available at www.phqscreeners.com. PHQ-9 (for MDD) scores of ≥10 and Generalized Anxiety Disorders (GAD-7) scores ≥10 have been associated with increased diabetes complications [368,369]. The DD scales can be accessed through https://diabetesdistress.org.
Screening instruments fall into 3 categories:
- Diabetes-specific measures, such as the Problem Areas in Diabetes (PAID) Scale or the Diabetes Distress Scales (DDS), including the T1D scale or either version of the T2D scales [370,371].
- Quality-of-life measures and function, such as the WHO-5 screening instrument [372] and Sheehan Disability scale.
- Depressive/anxiety symptoms, such as the Hospital Anxiety and Depression Scale (HADS) [373], the PHQ-9 [55,56], the Centre for Epidemiological Studies-Depression Scale (CES-D) [374], or the Beck Depression Inventory (BDI) [375].
Table 1 outlines the principal features and assessment methods to differentiate DD from MDD.
In addition, it is recommended that diabetes providers assess for attitudes that underlie PIR and FoH in those for whom it appears to be appropriate.
Table 3
Features of psychological treatments that can be integrated into diabetes treatment

Treatment
Psychosocial (non-pharmacological) treatments
Efforts to promote well-being to mitigate distress should be incorporated into diabetes management for all individuals [376]. Systematic reviews and meta-analyses have validated:
- Motivational interviewing [377,378]
- Cognitive behaviour therapy (CBT) [270,379]
- Acceptance and commitment therapy [380–385]
Furthermore, coping skills, self-efficacy enhancement, stress management [386,387], and family interventions [388–391] all have been shown to be helpful [18,392–394].
Case management by a provider working with the primary care provider and providing guideline-based, person-centred care resulted in improved A1C, lipid levels, blood pressure, and depression scores [384,395–397].
Individuals with depressive symptoms and/or psychiatric disorders benefit from professional interventions, either some form of psychotherapy or prescription medication. Evidence from systematic reviews of randomized controlled trials supports CBT and antidepressant medication, both individually or in combination [273,398,399], for treating depression. No evidence presently shows that the combination of CBT plus medication is superior to these treatments given individually. A pilot study of 50 people with T2D who initially had a moderate level of depression at baseline showed an improvement in the severity of their depression (moving to the mild range) with a 12-week intervention of 10 CBT sessions combined with exercise in the form of 150 minutes of aerobic activity weekly. This effect was sustained at 3 months [273].
Table 3
Among adults with T2D and subclinical depression, CBT resulted in reductions in DD and depressive symptoms compared to controls [405]. Lower diabetes regimen distress (produced by an intervention combining education, problem-solving, and support for accountability) led to improvements in medication adherence, physical activity, and decreased A1C over 1 year [406,407].
Recent research suggests that CBT can be used to address PIR by specifically addressing the beliefs that underlie it [33,106,408,409] (Figure 5
Since diabetes outcomes are heavily dependent on the sustained participation of the individual with the illness, motivational and behavioural change strategies can be effective. Diabetes care providers can enhance successful behaviour changes through motivational interviewing strategies, such as assessing/promoting readiness to change, having individuals weigh the advantages and disadvantages of making a self-management change, as well as encouraging their sense of self-efficacy/confidence in making the behavioural changes needed to improve their health [411–413]. Optimism and compassion from providers has also been shown to be helpful [414,415].
Although information and technology–based psychological treatments for the management of depression in people with diabetes appear to be effective in decreasing depressive symptomatology, this unfortunately may not translate into significant improvements in glycemic levels [416].
Psychological treatments delivered by non-specialists may be effective in improving glycemic levels. These treatments have some great potential of improving the quality of life for persons with T2D, particularly in low- and middle-income countries [417].
Finally, there is limited evidence to support art therapy and yoga in managing emotional distress and improving diabetes control [268,418].
Figure 5
Features of psychological insulin resistance/insulin refusal.
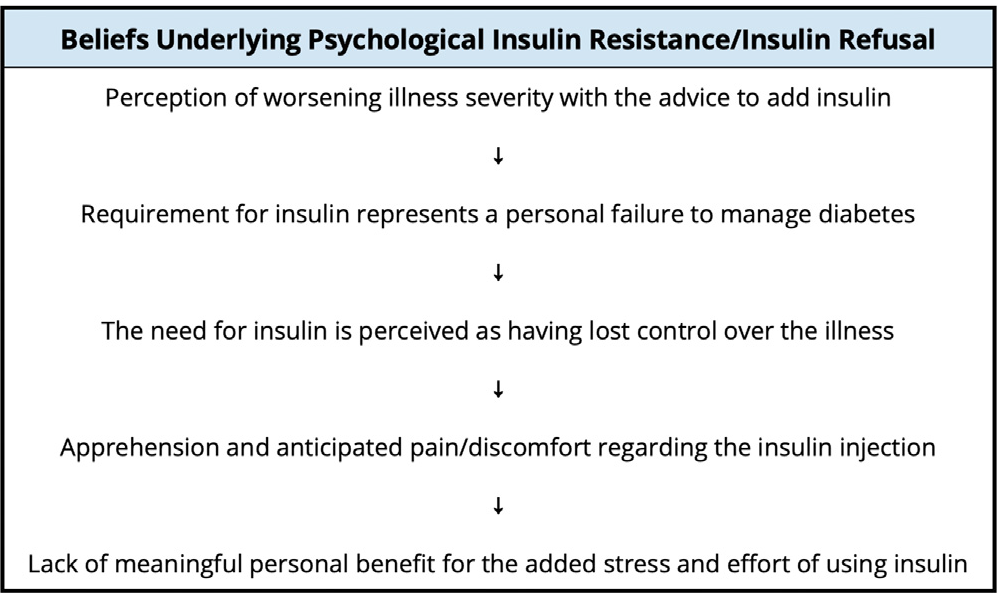
Pharmacological Treatments
Psychiatric medications treat a wide array of symptoms and conditions. They have the capability of making profound improvements in symptom severity and enhancing level of function and quality of life. For many people, prescription medications provide essential and even lifesaving treatments. Response (efficacy/effectiveness) and tolerability can only be established by an adequate trial of the pharmacological agent(s). These medications can also have effects on metabolic parameters, causing changes in weight, glycemic stability, and lipid profile, and have even been found to have immunomodulating effects [419–422].
Figure 6
Suggested cognitive behaviour therapy for fear of hypoglycemia.
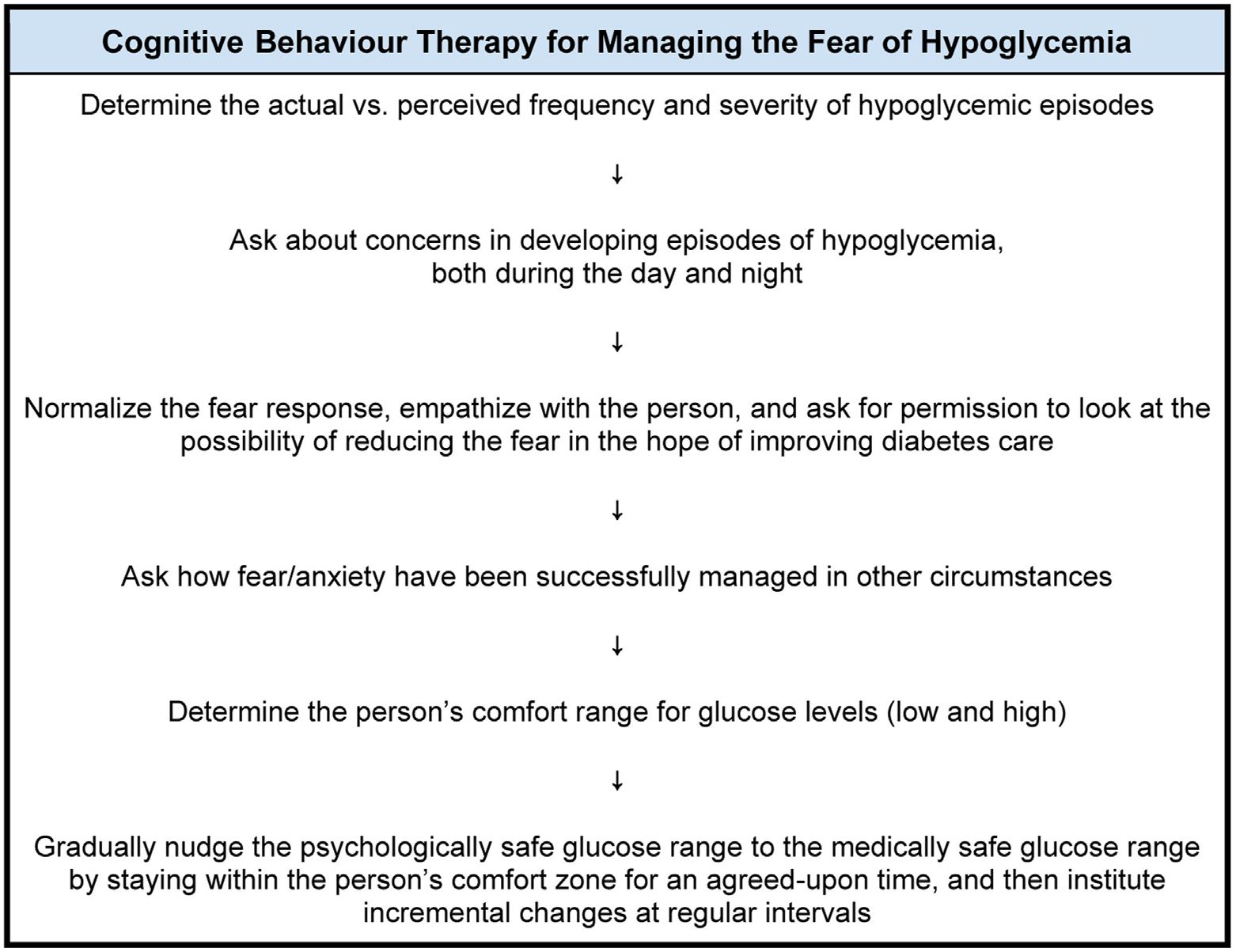
Antidepressant Medications
Introduction and overview
There are well over 20 antidepressants currently available in Canada. These are versatile medications that principally have an effect on monoamine transmission (serotonin, norepinephrine, or dopamine), with many having Health Canada-approved indications beyond MDD that include anxiety disorders, obsessive-compulsive and related disorders, trauma- and stressor-related disorders, and feeding and eating disorders.
Tricyclic antidepressants (TCAs) and monoamine oxidase inhibitors (MAOIs) generally have unfavourable side effects that are not tolerated well by people with diabetes (particularly sedation and weight gain) [423] and have been linked to an increased risk of developing diabetes [136,424,425].
Mirtazapine is a noradrenaline and serotonin specific antagonist (NaSSa) that contributes to the risk of weight gain, partly through its blockade of histamine receptors [423].
Selective serotonin reuptake inhibitors (SSRIs) currently comprise 6 medications that are available in Canada and are the most prescribed family of antidepressants. They are generally better tolerated and much safer to use than TCAs (particularly in overdoses) [426].
Serotonin-norepinephrine reuptake inhibitors (SNRIs) are generally more active on the serotonergic component than noradrenergic, with levomilnacipran having the strongest preference among the group for inhibiting norepinephrine reuptake. Bupropion is a norepinephrine and dopamine reuptake inhibitor. Desipramine is the TCA with the strongest action in blocking norepinephrine reuptake [427]. Glucose homeostasis theoretically could be disrupted by norepinephrine reuptake inhibition, but use of these medications has generally found this risk to be speculative, and agents causing norepinephrine reuptake inhibition can be used in treating depressive or anxious symptoms in people with diabetes [428].
Antidepressant use and diabetes risk
Depressive symptoms and their severity can act as confounding factors in assessing the relationship between antidepressants and diabetes risk. Antidepressants may have an impact on mental illness–related factors relevant to the risk for diabetes, such as physical activity and diet. There are several variables involved in the onset and control of depressive symptoms in people with T2D, which include:
- Presence/identification of depression symptoms
- Antidepressant medications
- Severity and duration of depressive symptoms
- Current diabetes medications
- Recreational substance use (alcohol, tobacco, cannabis, etc.)
- Weight/BMI [426]
Individuals who have depressive symptoms and disorders are at risk for developing T2D. It is challenging to separate what may be the metabolic effects of MDD versus the consequences to glucose regulation caused by antidepressant medication. Not surprisingly, there are discrepant data on the risk of diabetes.
Antidepressant use contributes to glucose dysregulation
Some reports [126,130–132] found that the administration of TCAs and SSRIs in moderate or higher doses appeared to increase the risk of glucose dysregulation or diabetes [94,424,429–432].
Length of antidepressant administration for MDD is another consideration. In one study, people treated with moderate-to-high antidepressant doses appeared to have an increased risk of developing diabetes [231].
Other studies have linked antidepressant use with an increased risk for T2D, particularly in people who take moderate-to-high doses and who have taken antidepressants for longer than 2 years. The risk was similar for TCAs and SSRIs [424,433,434].
Antidepressant use does not contribute to glucose dysregulation
Other studies have not found an association between antidepressants and diabetes risk [134,135]. One meta-analysis showed that A1C was 0.32% lower in people with diabetes and MDD who were treated with an antidepressant (and no additional psychological and pharmacological intervention) compared to those treated with placebo. This effect was shown to be more pronounced in pooled analysis of studies with only T2D compared to pooled data of all studies [434–436].
Short-term use of SSRIs appeared to stabilize or even reduce glucose levels, while the use of TCAs was associated with worsening of glycemic levels [437].
Another study even found that certain SSRIs appeared to improve metabolic parameters while others appeared to induce hyperglycemia and worsen glucose levels in people with both diabetes and MDD [438].
Ultimately, it may be that the risk of antidepressant-induced diabetes, which varies substantially even between medications of the same class, may not be a mechanism-based adverse effect, but due to an individual’s susceptibility [439].
Weight gain
A comprehensive review and meta-analysis looked at the effect of antidepressants on body weight [47]. These findings are incorporated in Table 7
Lipid abnormalities
Although weight gain is a risk factor for lipid abnormalities, the data presently indicate that these agents are unlikely to contribute to dyslipidemia [441].
Lithium
The most robust data linking lithium to diabetes is for diabetes insipidus [442], but it does not appear to increase the risk of developing diabetes mellitus. One study looked at the effect of lithium on fasting blood glucose over a 6-year span in people with bipolar disorder. This study concluded that lithium did not the development of diabetes mellitus [443].
Another analysis found that lithium had a lower-than-average risk among 102 medications for its potential contribution to the onset of T2D [444].
Increases in weight occur more often with lithium than placebo (31). If there is to be an increase in weight with lithium, it generally happens in the first 2 years. In contrast to antipsychotic-induced weight gain, a higher weight at the start of lithium treatment appears to predict a greater overall increase in weight. Weight increase is believed to result from increased appetite, lithium-induced hypothyroidism, and nephrogenic diabetes insipidus, leading to increased thirst (which may be satiated with sugary beverages) [445].
Anti-seizure medications
The effect of anti-seizure medications (often referred to as “mood stabilizers”) on weight change is not as common as with antipsychotics, but can still be significant. Weight increases occur more with valproate than with lamotrigine or topiramate [446], with three-quarters of people taking it reporting weight gain of up to approximately 6 kg [447].
Valproate, used in mental health for a variety of purposes, has also been found to contribute to the risk of insulin resistance [448].
Valproate is associated with weight gain in up to 50% of people taking it, and can be detected within 3 months after initiation. Average weight gain also appears to be approximately 6 kg, and does not appear to be dose dependent [449].
Carbamazepine appears to have a lower risk of weight gain than lithium or valproate [450].
Topiramate and lamotrigine (at higher doses) are weight neutral or may contribute to minor weight loss (found to be up to 1.2 kg) [449].
Antipsychotic medications
The family of medications known as “antipsychotics” can be subdivided into 3 generations. The first generation, also known as “typical” or “conventional” agents, largely function as dopamine receptor blockers and have demonstrated efficacy for reducing the more florid (also known as positive) signs of psychosis and, accordingly, received Health Canada–approved indications to treat psychotic disorders. However, these agents bind to a much wider variety of receptors than just dopamine and are useful in treating a wide array of symptoms and other (non-psychotic) conditions [423]. The second-generation antipsychotics, often called “atypical” or “novel,” have a more complex pharmacology, interacting principally with serotonin (5-HT2A) and dopamine receptors, but also binding to a wide array of other types of receptors. Several have Health Canada–approved indications for the manic/hypomanic/mixed phases of bipolar disorder in addition to psychotic disorders. However, the range of unofficial or non-approved uses is quite broad, and includes treating insomnia, anxiety, depressive symptoms, etc. The third-generation antipsychotics are known by their mechanism of action—partial agonists—and are described more fully below.
The first-generation antipsychotics cause a variety of adverse reactions, including prolactin elevation and a suite of neurological symptoms, including abnormal movements and movement disorders. They have also been shown to impair glucose metabolism and increase the risk of developing T2D [451].
Second-generation antipsychotics have generally been found to cause fewer adverse neurological reactions, but certain medications are capable of making a significant impact on metabolic parameters. One meta-analysis [452] found a 1.3-fold higher risk for developing diabetes in people with schizophrenia taking second-generation antipsychotics over first-generation medications. A more recent meta-analysis determined that there was insufficient evidence to draw a firm conclusion about this risk [453].
The first and second generations of antipsychotics are not homogeneous (as a family or class) for metabolic risks, and the use of any particular agent will have varying effects on a population basis.
Antipsychotic medication use during pregnancy has been found to be associated with a slightly higher risk of GDM [454]. Accordingly, this risk should be considered when making prescription decisions. If these medications are continued, then health-care providers should ensure enhanced monitoring of glycemic levels in these pregnant individuals in anticipation of the potential development of GDM over time [454,455].
Development of diabetes with antipsychotic medications
Olanzapine and clozapine have been associated with the greatest risk of glucose dysregulation or T2D in people with schizophrenia or bipolar disorder. Quetiapine, risperidone, and low-potency first-generation antipsychotics (e.g. chlorpromazine) are generally the agents that appear to have the next highest level of risk [456,457].
Antipsychotics have been reported to induce T2D even in people who do not experience weight increases from these medications [458,459].
There appears to be an indirect path to the development of T2D when weight increases occur, and possibly a more direct route via contributing to insulin resistance, which involves muscarinic cholinergic receptors. There are 5 subtypes of muscarinic receptors that have been identified presently, and M3 receptors in particular are thought to play a key role in the regulation of insulin secretion [458].
Olanzapine and clozapine, the 2 second-generation antipsychotic medications with the greatest risk of inducing diabetes, also have the highest M3 receptor-binding blocking affinity, interfering with insulin secretion and disrupting glucose homeostasis. This leads to insulin resistance and the development of T2D, especially during prolonged antipsychotic medication treatment [460].
Potential mechanisms for antipsychotic-induced diabetes
The major antipsychotic effect of first-generation or typical antipsychotics occurs by blocking dopamine D2 receptors in the mesolimbic, mesocortical, nigrostriatal, and tuberoinfundibular tracts. Both first- and second-generation antipsychotics have variable effects on muscarinic, histamine, and adrenergic receptors [461–463].
A large meta-analysis found that the prevalence of T2D in people prior to antipsychotic treatment was 2.9% and increased to an overall prevalence of 11.3% among those receiving treatment with a first- or second-generation antipsychotic. The reported risk of developing diabetes was highest in people taking olanzapine or clozapine and the lowest risk was associated with aripiprazole [88].
Antipsychotics can be obesogenic medications, with between 15%–72% of people taking second-generation antipsychotics experiencing weight gain of 7% or more. Increases in weight, should this occur, generally takes place in the first 6-8 weeks after initiation of antipsychotic therapy [464,465].
Antipsychotics can have a multifactorial contribution to increases in weight. They lead to increased appetite largely due to antagonism of the serotonin 5-HT2C receptors and/or histamine H1 receptors. Dopamine antagonism leads to increased craving and hedonic eating. Animal studies with atypical antipsychotics have reported alteration of gut microbiome. Finally, energy expenditure can be reduced due to the sedative effect of antipsychotics, further contributing increases in weight [458,466–469].
Although a major contributor, increases in weight are not the only factor contributing to an elevated risk of developing T2D. Antipsychotics are thought to cause downregulation of intracellular insulin signalling, leading to insulin resistance. At the same time, there seems to be a direct effect on the pancreatic β cells. Antagonism of the dopamine D2, serotonin 5-HT2C and muscarinic M3 receptors impairs β cell response to changes in blood glucose. In addition to the pharmacological effects, cell culture experiments have shown that antipsychotics increase apoptosis of β cells.
Increased weight and concomitant development of T2D is seen particularly in agents that exhibit high muscarinic M3 and histamine H1 receptor blockade [451] (Table 4
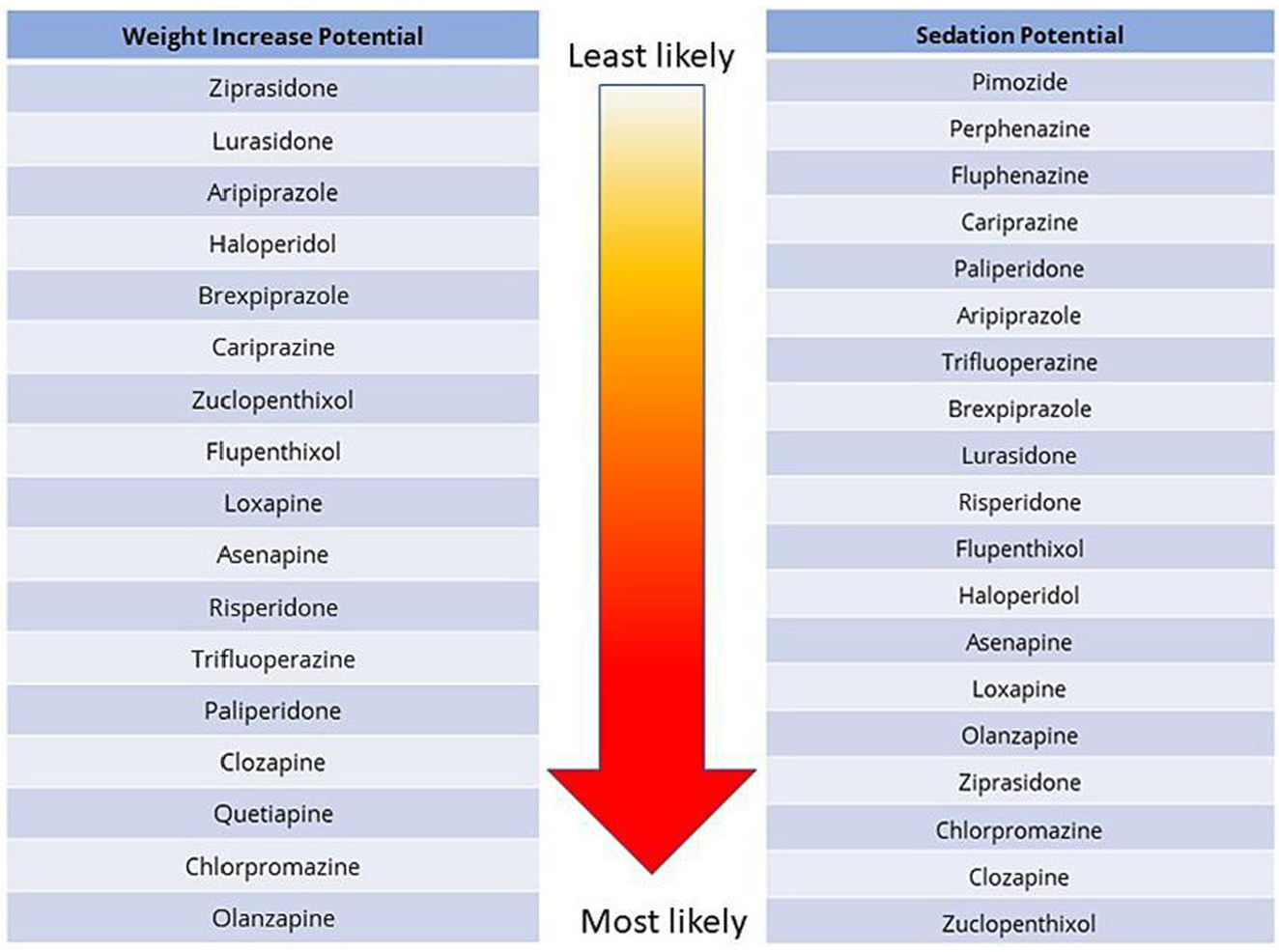
Increased weight associated with antipsychotic medications
Increased appetite and food intake, as well as delayed satiety signaling, are key physiological changes in antipsychotic-induced weight gain [458,459,473].
Antagonism at serotonin 5-HT2C and histamine H1 receptors appear to be involved in antipsychotic-induced weight increase, with H1 being the dominant of the 2 [446].
Clozapine and olanzapine, the antipsychotics with the highest risk for increases in weight, also have the highest affinities for 5-HT2C and H1 receptors. These are also key binding sites for mirtazapine and part of the reason that medication is notable for causing weight gain [458].
One systematic review/network meta-analysis compared the propensity of antipsychotics to cause weight increases and sedation, 2 particularly disadvantageous effects for people with diabetes [474]. While these adverse events were reported for people with schizophrenia who generally take higher doses of antipsychotic medications than those prescribed for adjunctive treatment of MDD, the relative ranking of the medications and weight increase/sedation potential is summarized in Table 5
Lipid changes associated with antipsychotic medications
Antipsychotics can cause lipid abnormalities, with adverse effects on triglycerides and cholesterol occurring early in the course of treatment (if they are to occur), possibly even before weight gain occurs [476,477].
Another systematic review/network meta-analysis investigated treatment-induced changes in body weight, BMI, and metabolic measures (fasting glucose, total cholesterol, LDL cholesterol, HDL cholesterol, and triglycerides) in people with schizophrenia who were treated with antipsychotic medication. Treatment duration varied from 2-13 weeks, with a median duration of 6 weeks. The results are summarized in Table 6
Serotonin-dopamine partial agonists/third-generation antipsychotics
Newer serotonin-dopamine partial agonists/third-generation antipsychotics have a reduced tendency to cause dysglycemia and weight increases. Compared to the other options, aripiprazole, brexpiprazole, and cariprazine have mild-to-modest histamine H1 antagonism, little serotonin 5-HT2C antagonism, and very little-to-no muscarinic M3 antagonism, giving them—as a family—the best receptor profile for reducing metabolic risks of the 3 generations of antipsychotics. They have the best overall metabolic profile in terms of minimizing increases in weight, glucose dysregulation, and lipid abnormalities of the antipsychotic families, though, as the newest generation, long-term metabolic data remains limited [479].
A systematic review of 32 antipsychotics used to treat schizophrenia (summarized in Table 5) found that for the risk of weight increase, the partial agonists were ranked 3, 5, and 6 in terms of being the least likely to increase weight. Similarly, when ranking the medications most likely to cause sedation, the partial agonists ranked 4, 11, and 14 in terms of causing the least amount of sedation [474].
Table 6
Antipsychotic adverse effects on metabolic parameters [478]
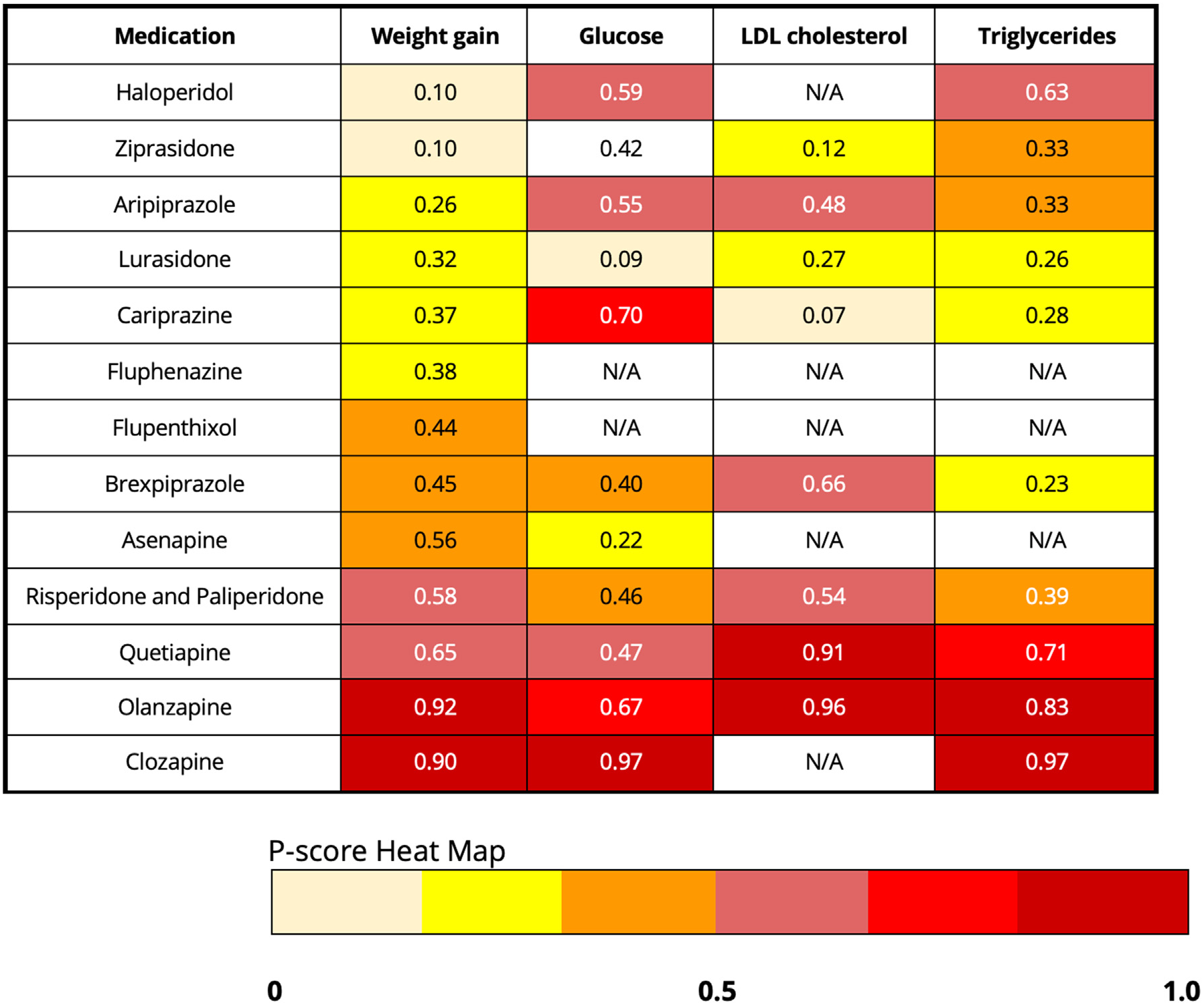
Footnote for Table 6: Results are ranked by propensity for increase in weight and reported with a P-score heat map, which ranks the likelihood of an adverse event on a scale from 0 to 1. A higher P-score indicates a larger increase in the metabolic parameter. The results were edited for antipsychotic medications presently available in Canada at the time of writing.
Aripiprazole
Aripiprazole (along with ziprasidone and lurasidone) was found, in several studies, to have little effect on fluctuations in body weight or glycemic levels [77,364,480-482].
In a systematic review of 40 population-based studies, aripiprazole appeared not to be associated with the occurrence of T2D, nor was it associated with an increased likelihood of developing dyslipidemia [483].
Use of aripiprazole and topiramate have evidence to support their use for managing antipsychotic-induced weight increases [449].
Augmentation with aripiprazole (to assist with symptom control in psychotic or mood disorders) can lead to a reduction in A1C levels, albeit minor [484].
Aripiprazole has also been reported to have a minor impact on body weight in children and adolescents [485].
Brexpiprazole
In a pooled analysis of phase 3 studies, the proportion of brexpiprazole-treated individuals with unfavourable shifts in metabolic parameters was low and like that of placebo-treated individuals, and unrelated to dose. In the short-term studies, mean (SD) increase in body weight was 1.2 (3.4) kg in the brexpiprazole group vs 0.2 (2.7) kg in the placebo group [486].
An open label study using brexpiprazole with data collected to 26 or 52 weeks involving an enrolment of over 1,000 people with schizophrenia found a mean change in body weight during long-term treatment of 2.0 (5.9) kg at week 26 and 3.2 (7.6) kg at week 52 [487].
Another pooled analysis of phase 3 studies looked at the effects caused by brexpiprazole used as an adjunct to treat MDD, specifically weight and metabolic parameters. Mean changes from baseline in lipids were small in the 6-week trials, with triglycerides showing the most significant increase. In most cases, the incidence of unfavourable shifts in metabolic parameters was lower than the incidence of favourable shifts. Mean body weight increase in the 6-week studies was 1.5 kg (with antidepressant being co-administered) compared to an antidepressant+placebo showing a weight increase of 0.3 kg. Studies of over 1 year found a mean body weight increase of 3.8 kg.
An analysis comparing changes in body weight using brexpiprazole and aripiprazole as monotherapy for schizophrenia or as adjunctive treatment to antidepressant treatment (MDD) summarized both short-term (4-6 week) trials and long-term (≤52 weeks) studies. Clinically relevant changes in body weight (≥7%) were similar for brexpiprazole and aripiprazole, with no statistically significant differences [488].
In short-term schizophrenia studies, the mean weight increase was 1.2 kg for brexpiprazole and 0.6 kg for aripiprazole. In short-term MDD studies (adjunctive to antidepressants), the mean weight increase was 1.5 kg for brexpiprazole and 1.6 kg for aripiprazole. In the long-term schizophrenia studies, at week 52, the mean weight increase was 2.1 kg for brexpiprazole and 3.0 kg for aripiprazole. In long-term MDD studies (adjunctive to antidepressant therapy), at week 52, the mean weight increase was 3.2 kg for brexpiprazole and 4.0 kg for aripiprazole [486].
Effects on glucose and lipids have generally been found to be minor. A mean gain of ∼1 kg greater than placebo was observed in short-term studies. The mean change in body weight decreased for both brexpiprazole and placebo in longer-term studies. Weight gain is generally reported to be higher in people taking brexpiprazole as an adjunct for MDD than for schizophrenia [489,490].
Cariprazine
A meta-analysis reviewing 9 randomized controlled studies involving over 4,300 people taking cariprazine found that people taking cariprazine were more likely to have a clinically significant increase in weight (RR 1.68, 95% CI 1.12–2.52), but no statistically significant differences in results were found in other metabolic parameters or cardiovascular-related events [491].
A double-blind, placebo-controlled phase 3 study examining the effectiveness of cariprazine in the depressed phase of bipolar disorder found that mean metabolic parameter changes were low, with a mean weight increase of ≤0.5 kg for all groups [492].
Antipsychotic summary
Switching to an antipsychotic with a lower tendency to cause weight gain can be an effective intervention for some, though reversal of any added weight does not always occur when medications are switched [473,493].
Recent guidelines have established the importance of mitigating potential increases in weight in individuals with T2D. These guidelines suggest that weight management is as important as maintaining glucose levels and cardiorenal risk reduction [494,495].
Given the ongoing change in the understanding of increases in weight and its association with the risk of developing T2D, a metabolically safer approach involves starting with medications that have a lower propensity for weight gain, and the partial agonists/third-generation antipsychotics as a family presently have the best overall data.
Antipsychotic use in children and adolescents
Antipsychotics should be used with caution in children and youth. One study found a 3-fold increased risk of diabetes in children and youth who were given antipsychotic medications compared to other classes of medications. The most frequently recorded diagnoses for which the medications were used were mood disorders, ADHD, and conduct disorder. The risk was already increased within the first year of medication administration, increased with cumulative lifetime dose, and remained elevated even 1 year after antipsychotic discontinuation [471,496,497].
Other studies have confirmed that children and adolescents using antipsychotics had a 2- to 3-fold increased risk of T2D[497,498], which was apparent within the first year of follow-up. Metformin has been shown to have a modest ability to reduce weight gain due to antipsychotic medication [499].
Although T2D seems rare in youth taking antipsychotic medications, cumulative risk and exposure-adjusted incidences were significantly higher than in healthy controls and controls with psychiatric conditions but not taking antipsychotic medications. Olanzapine treatment and antipsychotic exposure time were the main modifiable risk factors for T2D development in youth exposed to antipsychotic medications [500].
Children and adolescents appear to experience a greater degree of weight gain than adults when taking antipsychotic medication [501].
The medications that cause the greatest risk of weight gain in adults is the same as it is for children [502].
Children and adolescents who use antidepressants also appear to be at an elevated risk for developing diabetes [395,503].
Of note, atypical antipsychotic medications are often associated with increased weight, insulin resistance, impaired fasting glucose, and T2D in children and adolescents [504]. The risk of developing T2D may be higher in adolescents taking both antipsychotic and antidepressant medications, and should be considered when making psychopharmacological decisions to address mental health needs [505].
Effects of psychiatric medications on the risk for diabetes and weight gain
Should medical problems arise during a course of psychiatric medication, clinical judgement will dictate on a case-by-case basis whether healthy behaviour interventions, such as diet or physical activity, adding a medication to address the emergent issue (e.g. side effect or medical complication), or changing the psychiatric prescription, is the most reasonable step [506,507]. Resources are available to help clinicians quickly review the major side effect profiles of psychiatric medications [423,508].
The CATIE study investigated 4 aspects of the effectiveness of antipsychotic medications: efficacy, tolerability, emergence of medical problems, and individual choice [69]. The results indicated that some antipsychotic medications were more likely to cause weight to increase, worsen glycemic stability, and induce unfavourable changes in lipid profile (consistent with the results in Tables 5 and 6). All 4 aspects are important and reinforce the need for regular and comprehensive metabolic monitoring. Non-pharmacological interventions can be effective in reducing medication-associated weight gain and glucose changes [509].
Significant differences have been reported in the susceptibility to gain or lose weight with the same antipsychotic [31,38,477,510].
Irrespective of which antipsychotic medication is taken, changes can range from weight loss to weight neutrality to weight gain. Monozygotic twin and sibling studies indicate that genetic factors may be the dominant factor in medication-induced weight gain [473,510–513], with estimates as high as 60%-80% for antipsychotic-related weight gain [103].
Genetic factors control the expression of various receptors and compounds, including serotonin (5-HT2C) receptors, dopamine D2 receptors, brain-derived neurotrophic factor (BDNF), insulin-induced gene, leptin, and ghrelin (among many others) [77,447,458,473,478,514–516].
People with serious mental illnesses (SMI) usually experience weight gain, if it is to occur, early in the course of taking antipsychotics. The trajectory of weight gain usually flattens out within a year. The degree of weight gain in the first few weeks is usually a good predictor of the likelihood of longer-term weight gain and associated metabolic abnormalities [493].
Table 7
Psychiatric medications and risk of weight increase
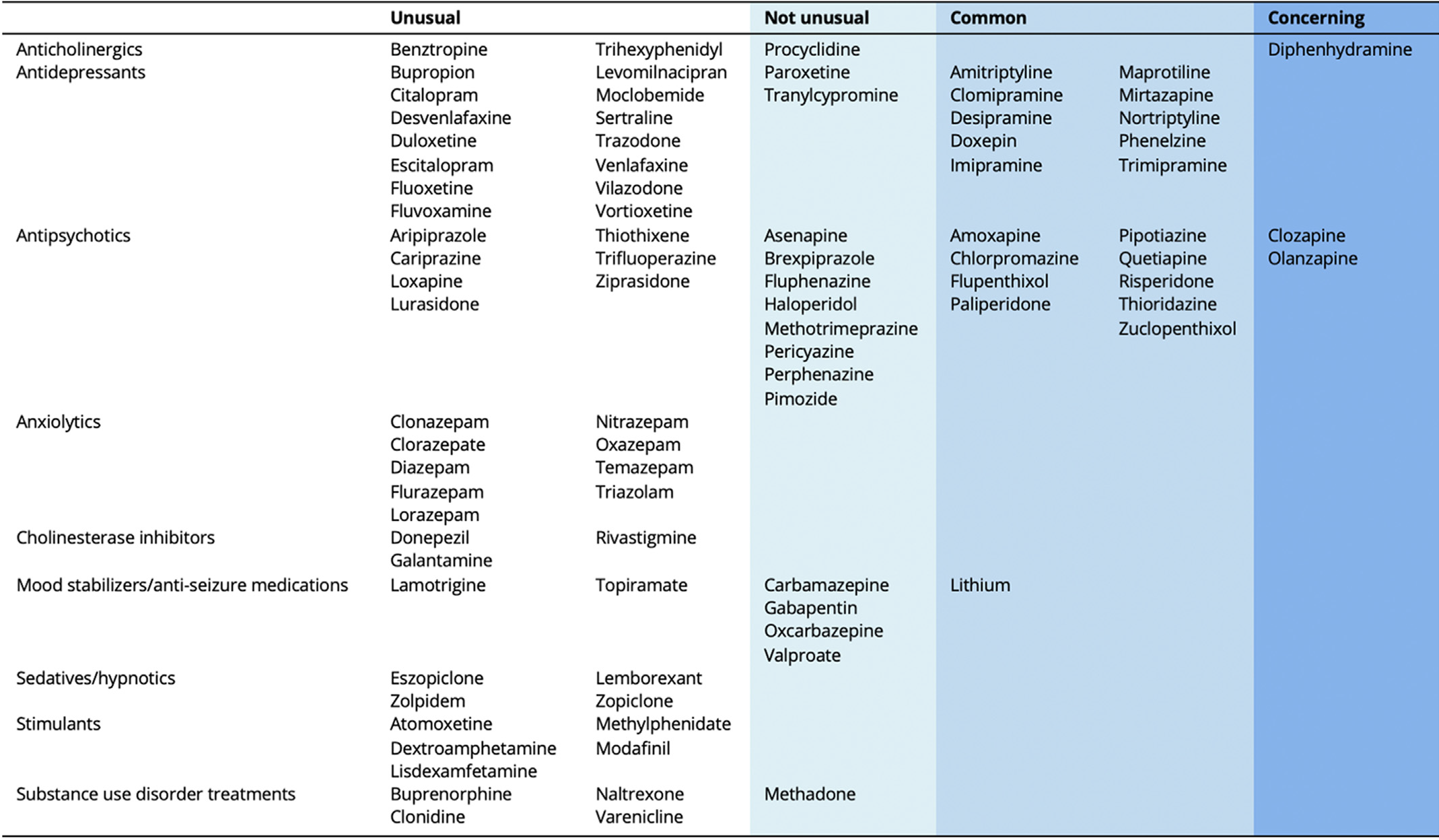
Monitoring Metabolic Risks
Health risks for people with SMI include:
- Increased weight/overweight/obesity
- Dyslipidemia
- Diabetes
- DKA
- Hypothyroidism (lithium only)
- Syndrome of inappropriate antidiuretic hormone release (SIADH)
- Hypertension
- Heart disease and stroke
- Sudden cardiac death
- Pneumonia
- Liver disease
- Leukocytopenia/agranulocytosis
- Thrombocytopenia
- Osteoporosis
- Kidney disease
- Movement disorders
People with SMI generally have a life expectancy 10-20 years shorter than the general population [517,518].
Despite the significant advances in cardiovascular health made in recent years, the benefits have not generally made an impact on people with SMI [519].
Many persons with SMI either do not have a primary care provider, or, if they do, may be inconsistent with keeping regular appointments and not benefit from cardiovascular monitoring. A shared care model does offer a possible solution, where psychiatric and primary care expertise is available in the same clinical space [520].
While lifestyle choices, genetics, and access to primary care all make an impact on metabolic risks in people with SMI, choice of psychiatric medication is the most easily addressed modifiable risk factor [77,441].
Metabolic syndrome is found at higher rates in individuals with psychiatric illnesses than in the general population [521,522]. Individuals with diabetes and comorbid psychiatric illnesses are at an elevated risk for developing metabolic syndrome, possibly due to a combination of the following factors [523]:
- Person-level factors (e.g. health behaviour choices, diet, tobacco consumption, recreational substance use, exercise, obesity, low degree of uptake of education programs)
- Illness factors (e.g. pro-inflammatory states from MDD or depressive symptoms, possible disease-related risks for developing diabetes) [524,525]
- Medication factors (e.g. psychotropic medications have variable effects on glycemic levels, weight fluctuations, and lipids)
- Environmental factors (e.g. access to health care, availability of screening and monitoring programs, social supports, education programs)
The main impact on lipid profile is an increase in triglyceride and total cholesterol levels, especially with clozapine, olanzapine, and quetiapine [69,526]. Table 7 lists the likelihood for weight gain with use of psychiatric medications. If a person is prescribed a medication that poses a higher risk for metabolic consequences, or has pre-existing uncontrolled dyslipidemia and is initiated on a higher-risk medication, then monitoring lipid levels as soon as 1 month is recommended. For all other circumstances, rechecking lipids at 3- to 6-month intervals is appropriate.
Regular, comprehensive monitoring of metabolic parameters is recommended for all persons who receive antipsychotic medications, whether or not they have diabetes. A1C was shown to be a more stable parameter in identifying psychiatric persons with diabetes [527]. Table 8
Because weight gain with medications tends to happen most quickly during the first few weeks, then slows and usually plateaus within 1 year [528], more frequent monitoring is recommended early in the course of treatment. Results indicate that the first year of antipsychotic treatment is a critical period for weight gain and metabolic abnormalities, as initial rapid weight gain is a significant predictor of the potential for long-term weight gain and obesity [458,529].
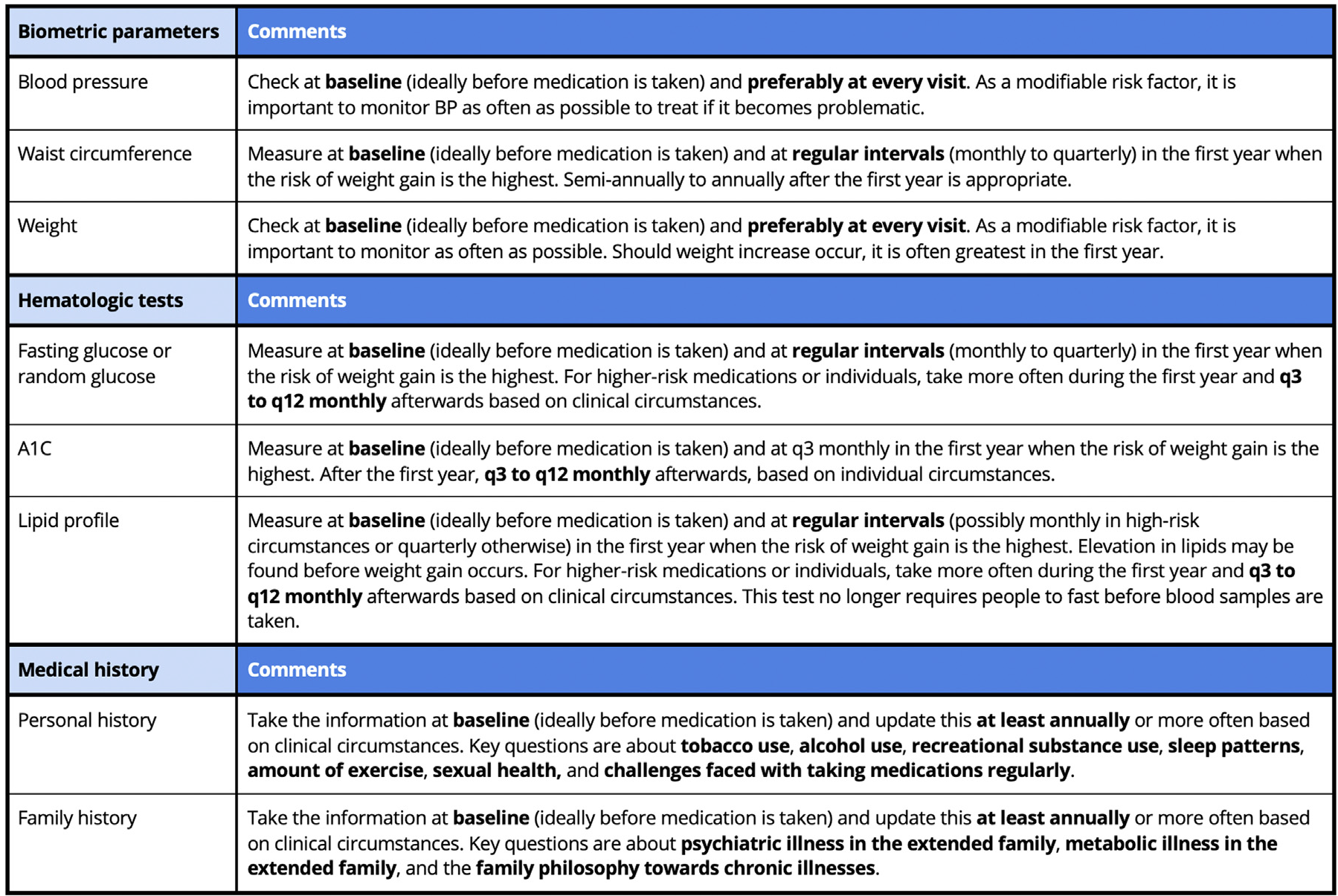
Recommendations
Reactions to the illness of diabetes
- Assess individuals with diabetes for psychological reactions to the diagnosis that may impair diabetes self-management [Grade D, Consensus].
- Health-care providers are advised to be aware of their own weight-based biases [Grade C, Level 3 [61]].
- Motivational interviewing techniques can be used to improve discussions focusing on weight to minimize weight-based stigma in health-care settings [Grade C, Level 3 [60,61]].
- Health-care providers are encouraged to regularly assess, counsel, and offer health-care resources to help individuals with diabetes to reduce the indirect and direct costs of diabetes management and improve self-management [Grade D, Level 4 [65]].
Screening
- Individuals with diabetes may be screened at each pregnancy-related follow-up visit for common psychiatric conditions (particularly mood and anxiety disorders), psychosocial stressors, and to assess social support [Grade D, Consensus].
- Children and adolescents with type 1 diabetes may benefit from screening at diagnosis and routine assessment to identify and address the mental health aspects of living with diabetes, specifically:
- Adolescents with type 1 diabetes may benefit from being regularly screened using non-judgemental questions about:
- Weight and body image concerns, and
- Dieting, binge eating, and insulin omission for weight loss [Grade D, Level 4 [256]].
- Children and adolescents with type 2 diabetes should be screened at diagnosis and regularly thereafter (at least twice per year) for major depressive disorder, binge eating disorder, and other psychosocial difficulties (e.g. diabetes distress and stigma) [Grade C, Level 3 [278,530]].
- Individuals with diabetes, as well as the parents or caregivers of youth with diabetes, should be screened when newly diagnosed, as well as regularly afterwards, for diabetes-related psychological distress and psychiatric disorders using validated self-report questionnaires or clinical interviews [Grade C, Level 3 [248,531]].
- Older people with diabetes should be screened for major depressive disorder and offered psychotherapy options, such as cognitive behaviour therapy, to improve physical health parameters, such as body weight [290], systolic blood pressure [290], glycemic management [289], and diabetes distress [289] [Grade B, Level 2].
- Health-care providers should use open and non-judgemental communication with adults with diabetes who are recreational substance users to facilitate implementation of strategies to reduce potential harm from substance use [Grade C, Level 3 [532]].
- People with diabetes may benefit from being screened for potential misuse of alcohol [Grade D, Level 4 [533]].
- For people with diabetes who have comorbid mental health concerns, inquiries about thoughts or plans for self-harm should be assessed regularly [Grade C, Level 3 [349]], and, when present, necessary steps should be taken to ensure the safety of the person [Grade D, Consensus].
Treatment
- For children and adolescents with type 1 diabetes, individual and family interventions, including mobile health (mHealth) and telemedicine resources, can be beneficial when included to address stress and/or diabetes-related conflict [Grade D, Consensus].
- Individuals with diabetes benefit from being counselled about the emotional and interpersonal impact of diabetes to improve their engagement in diabetes self-management recommendations [Grade D, Consensus].
- The following groups of people with diabetes may warrant referral to specialized mental health–care professionals:
- Significant distress related to diabetes management [Grade D, Consensus],
- Persistent fear of hypoglycemia [Grade D, Consensus],
- Psychological insulin resistance [Grade D, Consensus], and
- Psychiatric disorders (i.e. depression, anxiety, eating disorders) [Grade D, Consensus].
- Collaborative care by interprofessional teams should be provided for individuals with diabetes and depression to improve:
- Interventions may be provided by a multidisciplinary diabetes team (including a mental health professional) to support behaviour change and coping with lifestyle changes for individuals with diabetes [Grade D, Consensus].
- Psychosocial interventions should be integrated into diabetes care to improve adaptation to living with diabetes and engagement in self-management, including:
- Motivational interviewing [Grade A, Level 1A [378]],
- Cognitive behaviour therapy [Grade A, Level 1A [379]],
- Acceptance and commitment therapy [Grade A, Level 1 [380]],
- Stress management strategies [Grade A, Level 1A [18,392,393]],
- Coping skills training [Grade A, Level 1A [534] for type 2 diabetes; Grade B, Level 2 [535] for type 1 diabetes],
- Family therapy [Grade A, Level 1B [388,390,536]], and
- Case management [Grade A, Level 1 [394]].
- Cognitive behaviour therapy should be used to treat depression in individuals with depression alone [Grade B, Level 2 [137]] or in combination with antidepressant medication [Grade A, Level 1 [273,399]].
- People currently taking insulin therapy and who consume alcohol, cannabis, stimulants, or illicit opioids may be advised to:
- Accept counselling about the risk, prevention, recognition, and treatment of hypoglycemia, along with their support persons [Grade D, Consensus], and
- Monitor glucose levels frequently for glycemic excursions [alcohol [Grade C, Level 3 [297]]; other recreational substances [Grade C, Level 3 for T1D [297,319]]; Grade D, Consensus for T2D]].
- Antidepressant medication should be used to treat acute depression in people with diabetes [Grade A, Level 1 [136]] and for maintenance treatment to prevent recurrence of depression [Grade A, Level 1A [135]].
- People with diabetes or who are at risk for developing diabetes and who would benefit from an antipsychotic medication should be initially prescribed partial agonists/third-generation serotonin-dopamine modulators over first- and second-generation agents to reduce the chance of glycemic dysregulation, weight gain, or sedation [Grade C, Level 3 [474]].
Monitoring
- All persons (with or without diabetes) who are prescribed psychotropic medications (especially clozapine and olanzapine) should undergo metabolic monitoring at appropriate intervals to reduce the potential risk of adverse metabolic effects [Grade D, Consensus].
Abbreviations
A1C, glycated hemoglobin; BMI, body mass index; BP, blood pressure; CBT, cognitive behaviour therapy; CV, cardiovascular; DD, diabetes distress; DIP, diabetes in pregnancy; DKA, diabetic ketoacidosis; FoH, fear of hypoglycemia; GAD, generalized anxiety disorder; GDM, gestational diabetes mellitus; HR, hazard ratio; IR, insulin refusal; LDL-C, low-density lipoprotein cholesterol; MDD, major depressive disorder; PGM, pregestational/pre-pregnancy diabetes; PHQ-9, Patient Health Questionnaire; PIR, psychological insulin resistance; PPD, postpartum depression; PTSD, post-traumatic stress disorder; SMI, serious mental illness (generally includes schizophrenia and other psychotic disorders, bipolar disorder, and major depressive disorder); T1D, type 1 diabetes; T2D, type 2 diabetes
Author Disclosures
D.R. reports personal fees from AbbVie (legacy Allergan), Eisai, Janssen, Lundbeck, Otsuka, Sunovion and is the Chair and Founding Member of Master Clinician Alliance (a not-for-profit physician organization) outside of the submitted work. K.H reports no financial disclosures related to the submitted work. A.J. reports personal fees from Abbott, Acerus, Amgen, AstraZeneca, Bausch Health, Bayer, Boehringer Ingelheim, Care to Know, CCRN, Connected in Motion, CPD Network, Diabetes Canada, Dexcom, Eli Lilly, HLS Therapeutics, Insulet, Janssen, Master Clinician Alliance, MDBriefcase, Merck, Moderna, Novo Nordisk, Partners in Progressive Medical Education, Pfizer, PocketPills, Sanofi Aventis, Takeda, TimedRight and WebMD outside of the submitted work. J.K. reports personal fees from the Children with Diabetes, Connected In Motion, Diabetes Canada, American Diabetes Association and JDRF outside the submitted work. G.M. reports personal fees from HLS Therapeutics, Janssen, Lundbeck, Otsuka and Sunovion outside of the submitted work. O.M. receives grant/salary support from the Centre for Addiction and Mental Health and AMS Healthcare. M.V. reports personal fees from AbbVie, Bausch Health, Boehringer Ingelheim, CSL Behring, Merck, Novo Nordisk, Pfizer and Sanofi outside the submitted work.
Acknowledgments
Thank you to our external reviewers for their insightful feedback and the lending of their time and expertise: Jeffrey Habert MD CCFP FCFP Thomas Ungar MD, MEd, CCFP, FCFP, FRCPC, DABPN
References
- Digitale E. New research shows how to keep diabetics safer during sleep. SCOPE. Available from: https://scopeblog.stanford.edu/2014/05/08/new-research-keeps-diabetics-safer-during-sleep/.
- Moccia, L., et al., The Experience of Pleasure: A Perspective Between Neuroscience and Psychoanalysis. Front Hum Neurosci, 2018. 12: p. 359.
- Beck, A.T., A 60-Year Evolution of Cognitive Theory and Therapy. Perspect Psychol Sci, 2019. 14(1): p. 16-20.
- Shrivastava, S.R., Prateek Saurabh Shrivastava, and Jegadeesh Ramasamy, Role of self-care in management of diabetes mellitus. Journal of diabetes & Metabolic disorders, 2013. 12(1).
- Gonzalez JS, Tanenbaum ML, Commissariat PV. Psychosocial factors in medication adherence and diabetes self-management: Implications for research and practice. Am Psychol 2016; Oct;71(7):539-551. doi: 10.1037/a0040388.
- Snoek, F.J., et al., Monitoring of Individual Needs in Diabetes (MIND): baseline data from the Cross-National Diabetes Attitudes, Wishes, and Needs (DAWN) MIND study. Diabetes Care, 2011. 34(3): p. 601-603.
- Yilmaz, M., et al., Health Beliefs, Self-Care Behaviors and Quality of Life in Adults with Type 2 Diabetes. Florence Nightingale J Nurs, 2020. 28(2): p. 221-229.
- Swaleh, R.M. and C. Yu, "A Touch of Sugar": A Qualitative Study of the Impact of Health Beliefs on Type 1 and Type 2 Diabetes Self-Management Among Black Canadian Adults. Can J Diabetes, 2021. 45(7): p. 607-613 e2.
- Stewart, M., et al., Patient-centered medicine: transforming the clinical method. 2013: CRC press.
- Foot, H., et al., The necessity-concerns framework predicts adherence to medication in multiple illness conditions: A meta-analysis. Patient Education and Counseling, 2016. 99(5): p. 706-717.
- Nichols, J., et al., A Canadian Cross-Sectional Survey on Psychosocial Supports for Adults Living With Type 1 or 2 Diabetes: Health-Care Providers' Awareness, Capacity and Motivation. Can J Diabetes, 2018. 42(4): p. 389-394 e2.
- Vallis, M., et al., Equipping providers with principles, knowledge and skills to successfully integrate behaviour change counselling into practice: a primary healthcare framework. Public Health, 2018. 154: p. 70-78.
- Egede, L.E., P.J. Nietert, and D. Zheng, Depression and all-cause and coronary heart disease mortality among adults with and without diabetes. Diabetes Care, 2005. 28(6): p. 1339-1345.
- Hagger, V., et al., Diabetes Distress Among Adolescents with Type 1 Diabetes: a Systematic Review. Curr Diab Rep, 2016. 16(1): p. 9.
- Polonsky, W.H., et al., Assessing psychosocial distress in diabetes: development of the diabetes distress scale. Diabetes Care, 2005. 28(3): p. 626-631.
- Perrin, N., et al., Effectiveness of psychoeducational interventions for the treatment of diabetes-specific emotional distress and glycaemic control in people with type 2 diabetes: A systematic review and meta-analysis. Primary Care Diabetes, 2019. 13(6): p. 556-567.
- Fisher, L., et al., Understanding the sources of diabetes distress in adults with type 1 diabetes. Journal of Diabetes and its Complications, 2015. 29(4): p. 572-577.
- Miller, M., B. Knepper, and H. Young, Risk Factors Associated with 30-Day Readmission in Patients with Diabetic Foot Infections. Journal of the American Podiatric Medical Association, 2020. 110(6).
- Kenny, E., et al., Diabetes distress instruments in adults with Type 1 diabetes: A systematic review using the COSMIN (COnsensus-based Standards for the selection of health status Measurement INstruments) checklist. Diabetic medicine : a journal of the British Diabetic Association, 2021. 38(4): p. e14468.
- McMorrow, R., et al., Effect of routinely assessing and addressing depression and diabetes distress on clinical outcomes among adults with type 2 diabetes: a systematic review. BMJ Open, 2022. 12(5): p. e054650.
- Winchester, R.J., et al., Depressive symptoms, serious psychological distress, diabetes distress and cardiovascular risk factor control in patients with type 2 diabetes. Journal of Diabetes & its Complications, 2016. 30(2): p. 312-317.
- Strandberg, R.B., et al., Relationships of diabetes-specific emotional distress, depression, anxiety, and overall well-being with HbA1c in adult persons with type 1 diabetes. J Psychosom Res, 2014. 77(3): p. 174-179.
- Strandberg, R.B., et al., Longitudinal relationship between diabetes-specific emotional distress and follow-up HbA1c in adults with Type 1 diabetes mellitus. Diabetic Medicine, 2015. 32(10): p. 1304-1310.
- Dalsgaard, E.M., et al., Psychological distress, cardiovascular complications and mortality among people with screen-detected type 2 diabetes: follow-up of the ADDITION-Denmark trial. Diabetologia, 2014. 57(4): p. 710-717.
- Carper, M.M., et al., The differential associations of depression and diabetes distress with quality of life domains in type 2 diabetes. Journal of behavioral medicine, 2014. 37(3): p. 501-510.
- Pintaudi, B., et al., Correlates of diabetes-related distress in type 2 diabetes: Findings from the benchmarking network for clinical and humanistic outcomes in diabetes (BENCH-D) study. J Psychosom Res, 2015. 79(5): p. 348-354.
- Wardian, J. and F. Sun, Factors associated with diabetes-related distress: implications for diabetes self-management. Social work in health care, 2014. 53(4): p. 364-381.
- Bahrmann, A., et al., Psychological insulin resistance in geriatric patients with diabetes mellitus. Patient Education and Counseling, 2014. 94(3): p. 417-422.
- Holmes-Truscott, E., et al., Explaining psychological insulin resistance in adults with non-insulin-treated type 2 diabetes: The roles of diabetes distress and current medication concerns. Results from Diabetes MILES--Australia. Primary care diabetes, 2016. 10(1): p. 75-82.
- Khunti, K., et al., Therapeutic inertia in the treatment of hyperglycaemia in patients with type 2 diabetes: A systematic review. Diabetes Obes Metab, 2018. 20(2): p. 427-437.
- Polonsky, W.H., et al., Psychological insulin resistance in patients with type 2 diabetes. Diabetes Care, 2005. 28(10): p. 2543-2545.
- Hendrieckx, C., et al., Severe hypoglycaemia and its association with psychological well-being in Australian adults with type 1 diabetes attending specialist tertiary clinics. Diabetes Res Clin Pract, 2014. 103(3): p. 430-436.
- Nefs, G., et al., Fear of hypoglycaemia in adults with Type 1 diabetes: results from Diabetes MILES - The Netherlands. Diabetic Medicine, 2015. 32(10): p. 1289-1296.
- 2022 ISAPS international survey on aesthetic/cosmetic procedures performed in 2021. ISAPS. Accessed April XX, 2023. https://www.isaps.org/media/vdpdanke/isaps-global-survey_2021.pdf
- Hernandez CA, Freytag DL, Gold MH, et al. Clinical validation of the temporal lifting technique using soft tissue fillers. J Cosmet Dermatol. 2020;19(10):2529-2535.
- Gan SD, Itkin A, Wolpowitz D. Hyaluronic acid-induced alopecia: a novel complication. Dermatol Surg. 2013;39(11):1724-1725.
- Yang Q, Qiu L, Yi C, et al. Reversible alopecia with localized scalp necrosis after accidental embolization of the parietal artery with hyaluronic acid. Aesthet Plast Surg. 2017;41(3):695-699.
- Liu RF, Kuo TT, Chao YY, Huang YH. Alopecia with foreign body granulomas induced by Radiesse injection: A case report. J Cosmet Laser Ther. 2018;20(7-8):462-464.
- Khunkhet S, Rattananukrom T, Thanasarnaksorn W, Suchonwanit P. Alopecia induced by autologous fat injection into the temporal area: case report and review of the literature. Case Rep Dermatol. 2019;11(2):150-156.
- van den Elzen H, Schelke L, Velthuis P. Temporary hair loss after injection of hyaluronic acid filler. J Cosmet Dermatol. 2022;21(2):625-626.
- Li C, Zhang W. Vascular compromise and alopecia after hyaluronic acid filler injection in temple region. J Craniofac Surg. 2023;34(2):e128-e129.
- Coimbra DD, de Oliveira BS. Supra-auricular lifting with fillers: new technique. J Cosmet Dermatol. 2016;8(4):328-335.
- Casabona G, Frank K, Moellhoff N, et al. Full-face effects of temporal volumizing and temporal lifting techniques. J Cosmet Dermatol. 2020;19(11):2830-2837.
- Suwanchinda A, Webb KL, Rudolph C, et al. The posterior temporal supraSMAS minimally invasive lifting technique using soft-tissue fillers. J Cosmet Dermatol. 2018;17(4):617-624.
- Haidar R, Freytag M D DL, Frank K, et al. Quantitative analysis of the lifting effect of facial soft-tissue filler injections. Plast Reconstr Surg. 2021;147(5):765e-776e.
- Cotofana S, Gaete A, Hernandez CA, et al. The six different injection techniques for the temple relevant for soft tissue filler augmentation procedures-clinical anatomy and danger zones. J Cosmet Dermatol. 2020;19(7):1570-1579.
- Kang HG, Youn K-H, Kim I-B, Nam YS. Bilayered structure of the superficial facial fascia. Aesthet Surg J. 2017;37(6):627-636.
- DeLorenzi C. New high dose pulsed hyaluronidase protocol for hyaluronic acid filler vascular adverse events. Aesthet Surg J. 2017;37(7):814-825.
- Kato H, Kinoshita K, Saito N, et al. The effects of ischemia and hyperoxygenation on hair growth and cycle. Organogenesis. 2020;16(3):83-94.
- Fisher, L., et al., Clinical depression versus distress among patients with type 2 diabetes: not just a question of semantics. Diabetes Care, 2007. 30(3): p. 542-548.
- Fisher, L., R.E. Glasgow, and L.A. Strycker, The relationship between diabetes distress and clinical depression with glycemic control among patients with type 2 diabetes. Diabetes Care, 2010. 33(5): p. 1034-1036.
- Fisher, L., et al., Diabetes distress but not clinical depression or depressive symptoms is associated with glycemic control in both cross-sectional and longitudinal analyses. Diabetes Care, 2010. 33(1): p. 23-28.
- Kroenke, K. and R.L. Spitzer, The PHQ-9: a new depression diagnostic and severity measure. Psychiatric Annals, 2002. 32(9): p. 509-515.
- van Steenbergen-Weijenburg, K.M., et al., Validation of the PHQ-9 as a screening instrument for depression in diabetes patients in specialized outpatient clinics. BMC Health Serv Res, 2010. 10: p. 235.
- Brazeau, A.S., et al., Stigma and Its Association With Glycemic Control and Hypoglycemia in Adolescents and Young Adults With Type 1 Diabetes: Cross-Sectional Study. J Med Internet Res, 2018. 20(4): p. e151.
- Himmelstein, M.S. and R.M. Puhl, At multiple fronts: Diabetes stigma and weight stigma in adults with type 2 diabetes. Diabet Med, 2021. 38(1): p. e14387.
- Puhl, R.M., et al., Weight stigma and diabetes stigma in U.S. adults with type 2 diabetes: Associations with diabetes self-care behaviors and perceptions of health care. Diabetes Res Clin Pract, 2020. 168: p. 108387.
- Puhl, R.M., et al., Overcoming Weight Bias in the Management of Patients With Diabetes and Obesity. Clin Diabetes, 2016. 34(1): p. 44-50.
- Kushner, R.F., et al., An obesity educational intervention for medical students addressing weight bias and communication skills using standardized patients. BMC Medical Education, 2014. 14(53).
- Swiatoniowska-Lonc, N., et al., Psychosocial determinants of treatment adherence in patients with type 2 diabetes - a review. Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy, 2021. 14: p. 2701-2715.
- Kirkman, M.S., et al., Determinants of adherence to diabetes medications: findings from a large pharmacy claims database. Diabetes Care, 2015. 38(4): p. 604-609.
- Herkert D, V.P., Luo J, et al. , Cost-Related Insulin Underuse Among Patients With Diabetes. JAMA Intern Med, 2019. 179(1): p. 112-114
- Vitale, R.J., K. Wentzell, and L.M.B. Laffel, "Fear That One Day I May Not Be Able to Afford Insulin": The Emotional Burden of Diabetes Costs During Emerging Adulthood. Diabetes Technol Ther, 2022.
- Eby, E.L., et al, The association between adherence to insulin therapy and health care costs for adults with type 2 diabetes: Evidence from a US retrospective claims database. Journal of Managed Care & Specialty Pharmacy, 2020. 26(9).
- Diabetes Canada Clinical Practice Guidelines Expert, C., et al., Pharmacologic Glycemic Management of Type 2 Diabetes in Adults: 2020 Update. Can J Diabetes, 2020. 44(7): p. 575-591.
- Gaffney A., H., D., Woodhandler, S., Prevalence and Correlates of Patient Rationing of Insulin in the United States: A National Survey. Annals of Internal Medicine, 2022.
- Lieberman, J.A., et al., Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med, 2005. 353(12): p. 1209-1223.
- Brown, E.S., F.P. Varghese, and B.S. McEwen, Association of depression with medical illness: does cortisol play a role? Biol Psychiatry, 2004. 55(1): p. 1-9.
- McCreadie, R.G., Diet, smoking and cardiovascular risk in people with schizophrenia: descriptive study. Br J Psychiatry, 2003. 183: p. 534-539.
- Freeman SJ, R.W., Daneman D. , Type 1 diabetes and autism: is there a link? . Diabetes Care, 2005. 28: p. 925-926.
- Chen, M.H., et al., Risk of Developing Type 2 Diabetes in Adolescents and Young Adults With Autism Spectrum Disorder: A Nationwide Longitudinal Study. Diabetes Care, 2016. 39(5): p. 788-793.
- Bethin, K.E., et al., Autism spectrum disorder in children with Type 1 diabetes. Diabet Med, 2019. 36(10): p. 1282-1286.
- Anwar, A.J., J.D. Walker, and B.M. Frier, Type 1 diabetes mellitus and Down's syndrome: prevalence, management and diabetic complications. Diabetic Medicine, 1998. 15(2): p. 160-163.
- Chen, H.J., et al., Association of attention-deficit/hyperactivity disorder with diabetes: a population-based study. Pediatr Res, 2013. 73(4 Pt 1): p. 492-496.
- De Hert M, C.C., Bobes J et al. , Physical illness in patients with severe mental disorders. I. Prevalence, impact of medications and disparities in health care. World Psychiatry, 2011. 10: p. 52-77.
- Chesney, E., G.M. Goodwin, and S. Fazel, Risks of all-cause and suicide mortality in mental disorders: a meta-review. World Psychiatry, 2014. 13(2): p. 153-160.
- Vancampfort, D., et al., A meta-analysis of cardio-metabolic abnormalities in drug naive, first-episode and multi-episode patients with schizophrenia versus general population controls. World Psychiatry, 2013. 12(3): p. 240-250.
- Leucht, S., et al., Second-generation versus first-generation antipsychotic drugs for schizophrenia: a meta-analysis. The Lancet, 2009. 373(9657): p. 31-41.
- Mitchell, A.J., et al., Is the prevalence of metabolic syndrome and metabolic abnormalities increased in early schizophrenia? A comparative meta-analysis of first episode, untreated and treated patients. Schizophr Bull, 2013. 39(2): p. 295-305.
- Haupt, D.W. and J.W. Newcomer, Hyperglycemia and antipsychotic medications. J Clin Psychiatry, 2001. 62(Suppl 27): p. 15-26; discussion 40-1.
- Saddichha, S., et al., Diabetes and schizophrenia - effect of disease or drug? Results from a randomized, double-blind, controlled prospective study in first-episode schizophrenia. Acta Psychiatr Scand, 2008. 117(5): p. 342-347.
- Fleischhacker, W.W., et al., Metabolic risk factors in first-episode schizophrenia: baseline prevalence and course analysed from the European First-Episode Schizophrenia Trial. Int J Neuropsychopharmacol, 2013. 16(5): p. 987-995.
- McEvoy, J.P., et al., Prevalence of the metabolic syndrome in patients with schizophrenia: baseline results from the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) schizophrenia trial and comparison with national estimates from NHANES III. Schizophr Res, 2005. 80(1): p. 19-32.
- Wu, C.S., M.S. Lai, and S.S.F. Gau, Complications and mortality in patients with schizophrenia and diabetes: Populationbased cohort study. British Journal of Psychiatry, 2015. 207(5).
- Kouidrat, Y., et al., Advanced glycation end products and schizophrenia: a systematic review. Journal of Psychiatric Research, 2015. 66-67: p. 112-117.
- Vancampfort, D., et al., Diabetes mellitus in people with schizophrenia, bipolar disorder and major depressive disorder: a systematic review and large scale meta-analysis. World Psychiatry, 2016. 15(2): p. 166-174.
- Holt, R.I.G., and Alex J. Mitchell, Diabetes mellitus and severe mental illness: mechanisms and clinical implications. Nature Reviews Endocrinology, 2015. 11(2).
- Subramaniam, M., Siow-Ann Chong, and Elaine Pek, Diabetes mellitus and impaired glucose tolerance in patients with schizophrenia. The Canadian Journal of Psychiatry, 2003. 48(5).
- Taylor, D., et al. , Undiagnosed impaired fasting glucose and diabetes mellitus amongst inpatients receiving antipsychotic drugs. Journal of Psychopharmacology, 2005. 19(2).
- Voruganti, L.P., et al., Dysglycemia in a community sample of people treated for schizophrenia: the Diabetes in Schizophrenia in Central-South Ontario (DiSCO) study. Schizophr Res, 2007. 96(1-3): p. 215-222.
- Bai, Y.M., et al., Risk of developing diabetes mellitus and hyperlipidemia among patients with bipolar disorder, major depressive disorder, and schizophrenia: a 10-year nationwide population-based prospective cohort study. Journal of Affective Disorders, 2013. 150(1): p. 57-62.
- Mansur, R.B., et al., Impaired glucose metabolism moderates the course of illness in bipolar disorder. J Affect Disord, 2016. 195: p. 57-62.
- Calkin, C.V., et al., Insulin resistance and outcome in bipolar disorder. British Journal of Psychiatry, 2015. 206(1): p. 52-57.
- Kramer, N.E., et al., A clinical model for identifying an inflammatory phenotype in mood disorders. J Psychiatr Res, 2019. 113: p. 148-158.
- Anderson, R.J., et al., The prevalence of comorbid depression in adults with diabetes: a meta-analysis. Diabetes Care, 2001. 24(6): p. 1069-1078.
- Ali, S., et al., The prevalence of co-morbid depression in adults with Type 2 diabetes: a systematic review and meta-analysis. Diabet Med, 2006. 23(11): p. 1165-1173.
- Barnard, K.D., T.C. Skinner, and R. Peveler, The prevalence of co-morbid depression in adults with Type 1 diabetes: systematic literature review. Diabet Med, 2006. 23(4): p. 445-448.
- Egede, L.E., Diabetes, major depression, and functional disability among U.S. adults. Diabetes Care, 2004. 27(2): p. 421-428.
- Moussavi, S., et al., Depression, chronic diseases, and decrements in health: results from the World Health Surveys. Lancet, 2007. 370(9590): p. 851-858.
- Almeida, O.P., et al., Duration of diabetes and its association with depression in later life: The Health in Men Study (HIMS). Maturitas, 2016. 86: p. 3-9.
- Mezuk, B., et al., Is ignorance bliss? Depression, antidepressants, and the diagnosis of prediabetes and type 2 diabetes. Health Psychology, 2013. 32(3): p. 254-263.
- Rotella, F. and E. Mannucci, Depression as a risk factor for diabetes: a meta-analysis of longitudinal studies. Journal of Clinical Psychiatry, 2013. 74(1): p. 31-37.
- Yu, M., et al., Depression and Risk for Diabetes: A Meta-Analysis. Canadian Journal of Diabetes, 2015. 39(4): p. 266-272.
- Polonsky, W.H., et al., Are patients with type 2 diabetes reluctant to start insulin therapy? An examination of the scope and underpinnings of psychological insulin resistance in a large, international population. Curr Med Res Opin, 2011. 27(6): p. 1169-1174.
- Ludman, E.J., et al., Depression and diabetes symptom burden. Gen Hosp Psychiatry, 2004. 26(6): p. 430-436.
- Peyrot, M. and R.R. Rubin, Persistence of depressive symptoms in diabetic adults. Diabetes Care, 1999. 22(3): p. 448-452.
- Kikuchi, Y., et al., Association of severe hypoglycemia with depressive symptoms in patients with type 2 diabetes: The fukuoka diabetes registry. BMJ Open Diabetes Research and Care, 2015. 3 (1) (no pagination)(e000063).
- Werremeyer, A., et al., Disease control among patients with diabetes and severe depressive symptoms. Journal of Primary Care & Community Health, 2016. 7(2): p. 130-134.
- Engum, A., et al., Depression and diabetes: a large population-based study of sociodemographic, lifestyle, and clinical factors associated with depression in type 1 and type 2 diabetes. Diabetes Care, 2005. 28(8): p. 1904-1909.
- Li, C., et al., Prevalence and correlates of undiagnosed depression among U.S. adults with diabetes: the Behavioral Risk Factor Surveillance System, 2006. Diabetes Res Clin Pract, 2009. 83(2): p. 268-279.
- Katon, W.J., et al., Quality of depression care in a population-based sample of patients with diabetes and major depression. Med Care, 2004. 42(12): p. 1222-1229.
- Guo, M., et al., Metformin may produce antidepressant effects through improvement of cognitive function among depressed patients with diabetes mellitus. Clinical & Experimental Pharmacology & Physiology, 2014. 41(9): p. 650-656.
- Eaton, W.W., et al., Population-based study of first onset and chronicity in major depressive disorder. Arch Gen Psychiatry, 2008. 65(5): p. 513-520.
- Kendler, K.S., L.M. Karkowski, and C.A. Prescott, Causal relationship between stressful life events and the onset of major depression. Am J Psychiatry, 1999. 156(6): p. 837-841.
- Carvalhais, S.M., et al., The influence of socio-economic conditions on the prevalence of depressive symptoms and its covariates in an elderly population with slight income differences: the Bambui Health and Aging Study (BHAS). Int J Soc Psychiatry, 2008. 54(5): p. 447-456.
- Katon, W., et al., Depression and diabetes: factors associated with major depression at five-year follow-up. Psychosomatics, 2009. 50(6): p. 570-579.
- Bruce, D.G., W.A. Davis, and T.M. Davis, Longitudinal predictors of reduced mobility and physical disability in patients with type 2 diabetes: the Fremantle Diabetes Study. Diabetes care, 2005. 28(10): p. 2441-2447.
- Rubin, R.R., et al., Impact of intensive lifestyle intervention on depression and health-related quality of life in type 2 diabetes: the Look AHEAD Trial. Diabetes Care, 2014. 37(6): p. 1544-1553.
- Nyboe, L. and H. Lund, Low levels of physical activity in patients with severe mental illness. Nordic Journal of Psychiatry, 2013. 67(1): p. 43-46.
- Lawlor, D.A., G.D. Smith, and S. Ebrahim, Association of insulin resistance with depression: cross sectional findings from the British Women's Heart and Health Study. Bmj, 2003. 327(7428): p. 1383-1384.
- Timonen, M., et al., Insulin resistance and depressive symptoms in young adult males: findings from Finnish military conscripts. Psychosom Med, 2007. 69(8): p. 723-728.
- Okamura, F., et al., Insulin resistance in patients with depression and its changes during the clinical course of depression: minimal model analysis. Metabolism, 2000. 49(10): p. 1255-1260.
- Anagnostis, P., et al., Clinical review: the pathogenetic role of cortisol in the metabolic syndrome: a hypothesis. J Clin Endocrinol Metab, 2009. 94(8): p. 2692-2701.
- Pariante, C.M. and A.H. Miller, Glucocorticoid receptors in major depression: relevance to pathophysiology and treatment. Biol Psychiatry, 2001. 49(5): p. 391-404.
- Belmaker, R.H. and G. Agam, Major depressive disorder. N Engl J Med, 2008. 358(1): p. 55-68.
- Semenkovich, K., et al., Depression in type 2 diabetes mellitus: prevalence, impact, and treatment. Drugs, 2015. 75(6): p. 577-587.
- Ciechanowski, P.S., W.J. Katon, and J.E. Russo, Depression and diabetes: impact of depressive symptoms on adherence, function, and costs. Arch Intern Med, 2000. 160(21): p. 3278-3285.
- Lin, E.H., et al., Relationship of depression and diabetes self-care, medication adherence, and preventive care. Diabetes Care, 2004. 27(9): p. 2154-2160.
- Katon, W.J., et al., The association of comorbid depression with mortality in patients with type 2 diabetes. Diabetes Care, 2005. 28(11): p. 2668-2672.
- Zhang, X., et al., Depressive symptoms and mortality among persons with and without diabetes. Am J Epidemiol, 2005. 161(7): p. 652-660.
- Vancampfort, D., et al., Metabolic syndrome and metabolic abnormalities in patients with major depressive disorder: a meta-analysis of prevalences and moderating variables. Psychological medicine, 2014. 44(10): p. 2017-2028.
- Lustman, P.J., et al., Fluoxetine for depression in diabetes: a randomized double-blind placebo-controlled trial. Diabetes Care, 2000. 23(5): p. 618-623.
- Lustman, P.J., et al., Sertraline for prevention of depression recurrence in diabetes mellitus: a randomized, double-blind, placebo-controlled trial. Arch Gen Psychiatry, 2006. 63(5): p. 521-529.
- Lustman, P.J., et al., Effects of nortriptyline on depression and glycemic control in diabetes: results of a double-blind, placebo-controlled trial. Psychosom Med, 1997. 59(3): p. 241-250.
- Lustman, P.J., et al., Cognitive behavior therapy for depression in type 2 diabetes mellitus. A randomized, controlled trial. Ann Intern Med, 1998. 129(8): p. 613-621.
- Wade, C., et al., Increased anxiety symptoms in pediatric type 1 diabetes during the acute phase of COVID-19 lockdown. Journal of pediatric endocrinology & metabolism : JPEM, 2022.
- Azmiardi, A., et al., Low Social support and risk for depression in people with type 2 diabetes mellitus: A systematic review and meta-analysis. Journal of Preventive Medicine and Public Health, 2022. 55(1): p. 37.
- Hoerster, K.D., et al., PTSD is associated with poor health behavior and greater Body Mass Index through depression, increasing cardiovascular disease and diabetes risk among U.S. veterans. Prev Med Rep, 2019. 15: p. 100930.
- Katon, W., E.H. Lin, and K. Kroenke, The association of depression and anxiety with medical symptom burden in patients with chronic medical illness. Gen Hosp Psychiatry, 2007. 29(2): p. 147-155.
- Grigsby, A.B., et al., Prevalence of anxiety in adults with diabetes: a systematic review. J Psychosom Res, 2002. 53(6): p. 1053-1060.
- Bajor, L.A., et al., Associations between comorbid anxiety, diabetes control, and overall medical burden in patients with serious mental illness and diabetes. International Journal of Psychiatry in Medicine, 2015. 49(4): p. 309-320.
- Hasan, S.S., et al., Anxiety symptoms and the risk of diabetes mellitus in Australian women: evidence from 21-year follow-up. Public Health, 2016. 130: p. 21-28.
- Edwards, L.E. and B. Mezuk, Anxiety and risk of type 2 diabetes: evidence from the Baltimore Epidemiologic Catchment Area Study. J Psychosom Res, 2012. 73(6): p. 418-423.
- Chaturvedi, S.K., et al., More anxious than depressed: prevalence and correlates in a 15-nation study of anxiety disorders in people with type 2 diabetes mellitus. Gen Psychiatr, 2019. 32(4): p. e100076.
- Isomura, K., et al., Metabolic and Cardiovascular Complications in Obsessive-Compulsive Disorder: A Total Population, Sibling Comparison Study With Long-Term Follow-up. Biological psychiatry, 2018. 84(5): p. 324-331.
- Kelly, S.J. and M. Ismail, Stress and type 2 diabetes: a review of how stress contributes to the development of type 2 diabetes. Annual Review of Public Health, 2015. 36: p. 441-462.
- Farr, O.M., et al., Posttraumatic stress disorder, alone or additively with early life adversity, is associated with obesity and cardiometabolic risk. Nutrition Metabolism & Cardiovascular Diseases, 2015. 25(5): p. 479-488.
- Vaccarino, V., et al., Posttraumatic stress disorder and incidence of type-2 diabetes: a prospective twin study. Journal of Psychiatric Research, 2014. 56: p. 158-164.
- Goins, R.T., et al., Association of depressive symptomology and psychological trauma with diabetes control among older American Indian women: Does social support matter? J Diabetes Complications, 2017. 31(4): p. 669-674.
- Ram, D., H.G. Ashoka, and B. Gowdappa, Hyperglycemia associated dissociative fugue (organic dissociative disorder) in an elderly. J Family Med Prim Care, 2015. 4(3): p. 465-467.
- Baumert, J.e.a., A pattern of unspecific somatic symptoms as long-term premonitory signs of type 2 diabetes: findings from the population-based MONICA/ KORA cohort study, 1984-2009. Endocrine Disorders, 2014. 14(87).
- Clark, N.G., et al., Symptoms of diabetes and their association with the risk and presence of diabetes: findings from the Study to Help Improve Early evaluation and management of risk factors Leading to Diabetes (SHIELD). Diabetes Care, 2007. 30(11): p. 2868-2873.
- Crow, S., et al., Binge eating and other psychopathology in patients with type II diabetes mellitus. Int J Eat Disord, 2001. 30(2): p. 222-226.
- Colton, P.A., et al., Eating disorders in girls and women with type 1 diabetes: A longitudinal study of prevalence, onset, remission, and recurrence. Diabetes Care, 2015. 38(7): p. 1212-1217.
- Jones, J.M., et al., Eating disorders in adolescent females with and without type 1 diabetes: cross sectional study. BMJ, 2000. 320(7249): p. 1563-1566.
- Asamsama, O.H., et al., Bidirectional longitudinal study of type 2 diabetes and depression symptoms in black and white church going adults. J Diabetes Metab Disord, 2015. 14: p. 25.
- McCarthy, M., The thin ideal, depression and eating disorders in women. Behav Res Ther, 1990. 28(3): p. 205-215.
- Morse, S.A., et al., Isn't this just bedtime snacking? The potential adverse effects of night-eating symptoms on treatment adherence and outcomes in patients with diabetes. Diabetes Care, 2006. 29(8): p. 1800-1804.
- Harris, S.R., Maritza Carrillo, and Ken Fujioka, Binge-eating disorder and type 2 diabetes: A Review. Endocrine Practice, 2021. 27(2).
- Chevinsky, J.D., T.A. Wadden, and A.M. Chao, Binge Eating Disorder in Patients with Type 2 Diabetes: Diagnostic and Management Challenges. Diabetes Metab Syndr Obes, 2020. 13: p. 1117-1131.
- Coleman, S.E. and N. Caswell, Diabetes and eating disorders: an exploration of 'Diabulimia'. BMC Psychol, 2020. 8(1): p. 101.
- Anothaisintawee, T., et al., Sleep disturbances compared to traditional risk factors for diabetes development: Systematic review and meta-analysis. Sleep Med Rev, 2016. 30: p. 11-24.
- Feldman, H.A., et al., Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol, 1994. 151(1): p. 54-61.
- Lu, C.C., et al., Association of glycemic control with risk of erectile dysfunction in men with type 2 diabetes. J Sex Med, 2009. 6(6): p. 1719-1728.
- Enzlin, P., et al., Sexual dysfunction in women with type 1 diabetes: long-term findings from the DCCT/ EDIC study cohort. Diabetes Care, 2009. 32(5): p. 780-785.
- Olarinoye, J. and A. Olarinoye, Determinants of sexual function among women with type 2 diabetes in a Nigerian population. J Sex Med, 2008. 5(4): p. 878-886.
- Giugliano, F., et al., Determinants of erectile dysfunction in type 2 diabetes. Int J Impot Res, 2010. 22(3): p. 204-209.
- Varkonyi, T. and P. Kempler, Sexual dysfunction in diabetes, in Handbook of Clinical Neurology. 2014, Elsevier. p. 223-232.
- Abu Ali, R.M., et al., Sexual dysfunction in Jordanian diabetic women. Diabetes Care, 2008. 31(8): p. 1580-1581.
- Esposito, K., et al., Determinants of female sexual dysfunction in type 2 diabetes. Int J Impot Res, 2010. 22(3): p. 179-184.
- Enzlin, P., et al., Prevalence and predictors of sexual dysfunction in patients with type 1 diabetes. Diabetes Care, 2003. 26(2): p. 409-414.
- Maiorino, M.I., G. Bellastella, and K. Esposito, Diabetes and sexual dysfunction: Current perspectives. Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy, 2014. 7: p. 95-105.
- Gu Hong, W.C., et al., Effect of personality on blood glucose control in patients with type 1 diabetes. Endocrinologia, Diabetes y Nutricion, 2022.
- Maru, J., K. Millington, and J. Carswell, Greater Than Expected Prevalence of Type 1 Diabetes Mellitus Found in an Urban Gender Program. Transgend Health, 2021. 6(1): p. 57-60.
- Logel, S.N., M.T. Bekx, and J.L. Rehm, Potential association between type 1 diabetes mellitus and gender dysphoria. Pediatr Diabetes, 2020. 21(2): p. 266-270.
- Wierckx, K., et al., Prevalence of cardiovascular disease and cancer during cross-sex hormone therapy in a large cohort of trans persons: a case-control study. Eur J Endocrinol, 2013. 169(4): p. 471-478.
- Elbers JM., G.E., Teerlink T, Scheffer PG, Asscheman H, Seidell JC, et al. , Effects of sex steroids on components of the insulin resistance syndrome in transsexual subjects. Clin Endocrinol (Oxf). , 2003. 58(5): p. 526-571.
- Ellsworth, W. and G. Colon, Management of Medical Morbidities and Risk Factors Before Surgery: Smoking, Diabetes, and Other Complicating Factors. Seminars in Plastic Surgery, 2006. 20(4): p. 205-213.
- de Jonge, P., et al., Associations between DSM-IV mental disorders and diabetes mellitus: a role for impulse control disorders and depression. Diabetologia, 2014. 57(4): p. 699-709.
- Testa, G., et al., Transdiagnostic Perspective of Impulsivity and Compulsivity in Obesity: From Cognitive Profile to Self-Reported Dimensions in Clinical Samples with and without Diabetes. Nutrients, 2021. 13(12).
- Isidro, M.L. and S. Jorge, Recreational drug abuse in patients hospitalized for diabetic ketosis or diabetic ketoacidosis. Acta Diabetol, 2013. 50(2): p. 183-187.
- Lynch, C.P., et al., Impact of medical and psychiatric multi-morbidity on mortality in diabetes: emerging evidence. BMC Endocrine Disorders, 2014. 14: p. 68.
- Health, U.D.o. and H. Services, Smoking and diabetes (fact sheet) Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention. National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2014.
- Campagna, D., et al., Smoking and diabetes: dangerous liaisons and confusing relationships. Diabetol Metab Syndr, 2019. 11: p. 85.
- Faaitiiti, K.L. and D.C. Jupiter, Diabetes-Specific Dementia: A Structured Literature Review of Cognitive Assessment Methods. The Journal of Foot and Ankle Surgery, 2022. 61(2): p. 401-409.
- Carr, A.L., et al., Depression as a risk factor for dementia in older people with type 2 diabetes and the mediating effect of inflammation. Diabetologia, 2021. 64(2): p. 448-457.
- Hackett, R.A., et al., Hostility and physiological responses to acute stress in people with type 2 diabetes. Psychosom Med, 2015. 77(4): p. 458-466.
- Nefs, G., et al., Type D personality, suboptimal health behaviors and emotional distress in adults with diabetes: results from Diabetes MILES-The Netherlands. Diabetes Research & Clinical Practice, 2015. 108(1): p. 94-105.
- Dybdal, D., et al., Increasing risk of psychiatric morbidity after childhood onset type 1 diabetes: a population-based cohort study. Diabetologia, 2018. 61(4): p. 831-838.
- Ehrenthal, J.C., et al., Levels of personality functioning and not depression predict decline of plasma glucose concentration in patients with type 2 diabetes mellitus. Diabetes Research and Clinical Practice, 2019. 151: p. 106-113.
- Cukic, I. and A. Weiss, Personality and diabetes mellitus incidence in a national sample. Journal of Psychosomatic Research, 2014. 77(3): p. 163-168.
- Widiger, T.A. and J.R. Oltmanns, Neuroticism is a fundamental domain of personality with enormous public health implications. World Psychiatry, 2017. 16(2): p. 144-145.
- McLeod, S.A., Type A personality, in Simply Psychology. 2017.
- Sanchez-Urbano, C., M.J. Pino, and C. Herruzo, Personality Prototypes in People with Type 1 Diabetes and Their Relationship with Adherence. Int J Environ Res Public Health, 2021. 18(9).
- Hoffmann, M., et al., Depression as a risk factor for mortality in individuals with diabetes: a meta-analysis of prospective studies. PLoS ONE [Electronic Resource], 2013. 8(11): p. e79809.
- Park, M., W.J. Katon, and F.M. Wolf, Depression and risk of mortality in individuals with diabetes: a meta-analysis and systematic review. General Hospital Psychiatry, 2013. 35(3): p. 217-225.
- Chwastiak, L.A., et al., The effect of serious mental illness on the risk of rehospitalization among patients with diabetes. Psychosomatics, 2014. 55(2): p. 134-143.
- Novak, M., et al., Increased risk of incident chronic kidney disease, cardiovascular disease, and mortality in patients with diabetes with comorbid depression. Diabetes Care, 2016. 39(11): p. 1940-1947.
- Munoz, F.A., et al., Increased length of stay and hospital charges in adolescents with type 1 diabetes and psychiatric illness. J Pediatr Endocrinol Metab, 2021. 34(2): p. 183-186.
- Zou, Y., et al., Depression and Retinopathy in Patients With Type 2 Diabetes Mellitus: A Meta-Analysis. Psychosomatic medicine, 2021. 83(3): p. 239-246.
- Krein, S.L., et al, Diabetes treatment among VA patients with comorbid serious mental illness. Psychiatric services (Washington, D.C.), 2006. 57(7).
- Siddiqui, N., et al., Hospital length of stay variation and comorbidity of mental illness: a retrospective study of five common chronic medical conditions. BMC Health Serv Res, 2018. 18(1): p. 498.
- Mehta, G., et al, Impact of Diabetes on inpatient length of stay in adult mental health services in a community hospital setting: A retrospective cohort study. Canadian Journal of Diabetes, 2022.
- Potter, L.C., et al., Categories and health impacts of intimate partner violence in the World Health Organization multi-country study on women's health and domestic violence. Int J Epidemiol, 2021. 50(2): p. 652-662.
- OuYang, H., et al., Associations between Gestational Diabetes and Anxiety or Depression: A Systematic Review. J Diabetes Res, 2021. 2021: p. 9959779.
- Wilson, C.A., et al., Is there an increased risk of perinatal mental disorder in women with gestational diabetes? A systematic review and meta-analysis. Diabet Med, 2020. 37(4): p. 602-622.
- Beka, Q., et al., Development of Perinatal Mental Illness in Women With Gestational Diabetes Mellitus: A Population-Based Cohort Study. Can J Diabetes, 2018. 42(4): p. 350-355 e1.
- Minschart, C., et al., Antenatal Depression and Risk of Gestational Diabetes, Adverse Pregnancy Outcomes, and Postpartum Quality of Life. The Journal of clinical endocrinology and metabolism, 2021. 106(8): p. e3110-e3124.
- Quansah, D.Y., et al., Cardiometabolic and mental health in women with early gestational diabetes mellitus: a prospective cohort study. The Journal of Clinical Endocrinology & Metabolism, 2022. 107(3): p. e996-e1008.
- Ross, G.P., et al., Relationship between depression and diabetes in pregnancy: A systematic review. World Journal of Diabetes, 2016. 7(19): p. 554-571.
- Hinkle, S.N., et al., A longitudinal study of depression and gestational diabetes in pregnancy and the postpartum period. Diabetologia, 2016. 59(12): p. 2594-2602.
- Miller, N.E., et al., Impact of gestational diabetes diagnosis on concurrent depression in pregnancy. Journal of Psychosomatic Obstetrics and Gynecology, 2021. 42(3): p. 190-193.
- Delanerolle, G., et al., A systematic review and meta-analysis of gestational diabetes mellitus and mental health among BAME populations. EClinicalMedicine, 2021. 38: p. 101016.
- Maguire PA, Reay RE, Nolan CJ, and Looi JC. The single-item Self-Rated Mental Health Question in women with gestational diabetes mellitus. Australasian Psychiatry: Bulletin of Royal Australian and New Zealand College of Psychiatrists 2022; 30(4): 472-475
- Hamidi, F., et al., The effectiveness of mindfulness-based training on anxiety in pregnant women with gestational diabetes. Family Medicine and Primary Care Review, 2020. 22(4): p. 279-283.
- Molyneaux, E., et al., Do elevated symptoms of depression predict adherence and outcomes in the UPBEAT randomised controlled trial of a lifestyle intervention for obese pregnant women? BMC pregnancy and childbirth, 2018. 18(1): p. 378.
- Kumah-Crystal, Y. and S. Mulvaney, Utilization of blood glucose data in patient education. Current Diabetes Reports, 2013. 13(6): p. 886-893.
- Do, N.C., et al., Quality of life, anxiety and depression symptoms in early and late pregnancy in women with pregestational diabetes. Acta obstetricia et gynecologica Scandinavica, 2017. 96(2): p. 190-197.
- Brown, H.K., et al., Pre-Pregnancy Diabetes and Perinatal Mental Illness: A Population-Based Latent Class Analysis. American journal of epidemiology, 2019.
- Callesen, N.F., et al., Mental health in early pregnancy is associated with pregnancy outcome in women with pregestational diabetes. Diabetic Medicine, 2015. 32(11): p. 1484-1491.
- Silverman, M.E., et al., The risk factors for postpartum depression: a population-based study. Depress Anxiety, 2017. 34(2): p. 178-187.
- Lee, K.W., et al., Diabetes in Pregnancy and Risk of Antepartum Depression: A Systematic Review and Meta-Analysis of Cohort Studies. International journal of environmental research and public health, 2020. 17(11).
- Egan, A.M., et al., Diabetes in pregnancy: Worse medical outcomes in type 1 diabetes but worse psychological outcomes in gestational diabetes. QJM, 2017. 110(10): p. 721-727.
- Borges, R.d.P., et al., Impact of the COVID-19 pandemic on mental health of pregnant women with diabetes mellitus and hypertension. Revista da Associacao Medica Brasileira (1992), 2021. 67(9): p. 1268-1273.
- Ward, C., et al., 1166: Characterization of diabetes distress in pregnancy: A pilot study. American Journal of Obstetrics and Gynecology, 2020. 222(1 Supplement): p. S717-S718.
- Langer, N. and O. Langer, Comparison of pregnancy mood profiles in gestational diabetes and preexisting diabetes. Diabetes Educ, 2000. 26(4): p. 667-672.
- Levy-Shiff, R., et al., Maternal adjustment and infant outcome in medically defined high-risk pregnancy. Developmental Psychology, 2002. 38(1): p. 93-103.
- Fogel, N.R. and J. Weissberg-Benchell, Preventing poor psychological and health outcomes in pediatric type 1 diabetes. Curr Diab Rep, 2010. 10(6): p. 436-443.
- Lawrence, J.M., et al., Prevalence and correlates of depressed mood among youth with diabetes: the SEARCH for Diabetes in Youth study. Pediatrics, 2006. 117(4): p. 1348-1358.
- Hood, K.K., et al., Depressive symptoms in children and adolescents with type 1 diabetes: association with diabetes-specific characteristics. Diabetes Care, 2006. 29(6): p. 1389-1391.
- Northam, E.A., et al., Psychiatric morbidity and health outcome in Type 1 diabetes--perspectives from a prospective longitudinal study. Diabet Med, 2005. 22(2): p. 152-157.
- Kakleas, K., et al., Psychosocial problems in adolescents with type 1 diabetes mellitus. Diabetes Metab, 2009. 35(5): p. 339-350.
- McDonnell, C.M., et al., Hyperglycemia and externalizing behavior in children with type 1 diabetes. Diabetes Care, 2007. 30(9): p. 2211-2215.
- Rees, S.E., et al., Engaging Patients and Clinicians in Establishing Research Priorities for Gestational Diabetes Mellitus. Canadian Journal of Diabetes., 2016. 14.
- Verburg, P.E., et al., Seasonality of gestational diabetes mellitus: A South Australian population study. BMJ Open Diabetes Research and Care, 2016. 4 (1) (no pagination)(e000286).
- Walmer, R., et al., MENTAL HEALTH DISORDERS SUBSEQUENT to GESTATIONAL DIABETES MELLITUS DIFFER by RACE/ETHNICITY. Depression and Anxiety, 2015. 32(10): p. 774-782.
- Chida, Y. and M. Hamer, An association of adverse psychosocial factors with diabetes mellitus: a meta-analytic review of longitudinal cohort studies. Diabetologia, 2008. 51(12): p. 2168-2178.
- Stewart, S.M., et al., Depressive symptoms predict hospitalization for adolescents with type 1 diabetes mellitus. Pediatrics, 2005. 115(5): p. 1315-1319.
- Garrison, M.M., W.J. Katon, and L.P. Richardson, The Impact of psychiatric comorbidities on readmissions for diabetes in youth. Diabetes Care, 2005. 28(9): p. 2150-2154.
- Hassan, K., et al., The role of socioeconomic status, depression, quality of life, and glycemic control in type 1 diabetes mellitus. J Pediatr, 2006. 149(4): p. 526-531.
- Cunningham, N.R., et al., From caregiver psychological distress to adolescent glycemic control: the mediating role of perceived burden around diabetes management. J Pediatr Psychol, 2011. 36(2): p. 196-205.
- Butler, J.M., et al., Maternal parenting style and adjustment in adolescents with type I diabetes. J Pediatr Psychol, 2007. 32(10): p. 1227-1237.
- Jaser, S.S., et al., Mediators of depressive symptoms in children with type 1 diabetes and their mothers. J Pediatr Psychol, 2008. 33(5): p. 509-519.
- Eckshtain, D., et al., The effects of parental depression and parenting practices on depressive symptoms and metabolic control in urban youth with insulin dependent diabetes. J Pediatr Psychol, 2010. 35(4): p. 426-435.
- Chapman, K., et al., Emergency glucagon: a focused review of psychosocial experiences of rescue drugs for type 1 diabetes. Current diabetes reports, 2022. 22(4): p. 189-197.
- Zhang, L., et al., Related factors associated with fear of hypoglycemia in parents of children and adolescents with type 1 diabetes - A systematic review. J Pediatr Nurs, 2022. 66: p. 125-135.
- Abitbol, L. and M.R. Palmert, When Low Blood Sugars Cause High Anxiety: Fear of Hypoglycemia Among Parents of Youth With Type 1 Diabetes Mellitus. Canadian Journal of Diabetes, 2021. 45(5): p. 403.
- Hood, K.K., The influence of caregiver depressive symptoms on proxy report of youth depressive symptoms: a test of the depression-distortion hypothesis in pediatric type 1 diabetes. Journal of Pediatric Psychology, 2009. 34(3): p. 294-303.
- Cobry, E.C., et al., Improvements in Parental Sleep, Fear of Hypoglycemia, and Diabetes Distress With Use of an Advanced Hybrid Closed-Loop System. Diabetes Care, 2022. 45(5): p. 1292-1295.
- Cameron, L.D., M.J. Young, and D.J. Wiebe, Maternal trait anxiety and diabetes control in adolescents with type 1 diabetes. J Pediatr Psychol, 2007. 32(7): p. 733-744.
- Nguyen, L.A., et al., Depression and anxiety in adolescents with type 1 diabetes and their parents. Pediatric Research, 2022. 91(1): p. 188-196.
- Rydall, A.C., et al., Disordered eating behavior and microvascular complications in young women with insulin-dependent diabetes mellitus. N Engl J Med, 1997. 336(26): p. 1849-1854.
- Young-Hyman, D.L. and C.L. Davis, Disordered eating behavior in individuals with diabetes: importance of context, evaluation, and classification. Diabetes Care, 2010. 33(3): p. 683-689.
- Bachle, C., et al., Symptoms of eating disorders and depression in emerging adults with early-onset, long-duration type 1 diabetes and their association with metabolic control. PLoS ONE, 2015. 10 (6) (no pagination)(e0131027).
- Butwicka, A., et al., Psychiatric disorders and health-related quality of life in children with type 1 diabetes mellitus. Psychosomatics, 2016. 57(2): p. 185-193.
- Stahl-Pehe, A., et al., Screening for generalized anxiety disorder (GAD) and associated factors in adolescents and young adults with type 1 diabetes: Cross-sectional results of a Germany-wide population-based study. Diabetes Research and Clinical Practice, 2022. 184: p. 109197.
- Chao, A.M., et al., General life and diabetes-related stressors in early adolescents with type 1 diabetes. Journal of Pediatric Health Care, 2016. 30(2): p. 133-142.
- Schwartz, D.D., et al., Early risk factors for nonadherence in pediatric type 1 diabetes: a review of the recent literature. Curr Diabetes Rev, 2010. 6(3): p. 167-183.
- Cameron, F.J., et al., Routine psychological screening in youth with type 1 diabetes and their parents: a notion whose time has come? Diabetes Care, 2007. 30(10): p. 2716-2724.
- Garey, C.J., et al., The association between depression symptom endorsement and glycemic outcomes in adolescents with type 1 diabetes. Pediatric diabetes, 2022. 23(2): p. 248-257.
- Bisno, D.I., et al., Virtual Group Appointments Reduce Distress and Improve Care Management in Young Adults with Type 1 Diabetes. Journal of diabetes science and technology, 2021: p. 19322968211035768.
- Garner, K., et al., Digital health interventions for improving mental health outcomes and wellbeing for youth with type 1 diabetes: A systematic review. Pediatric diabetes, 2022. 23(2): p. 258-269.
- Huang, M.-X., M.-C. Wang, and B.-Y. Wu, Telehealth Education via WeChat Improves the Quality of Life of Parents of Children with Type-1 Diabetes Mellitus. Applied Clinical Informatics, 2022. 13(01): p. 263-269.
- Garvey, K.C., et al., Health Care Transition Preparation and Experiences in a U.S. National Sample of Young Adults With Type 1 Diabetes. Diabetes Care, 2017. 40(3): p. 317-324.
- Garvey, K.C., et al., Health care transition in patients with type 1 diabetes: young adult experiences and relationship to glycemic control. Diabetes Care, 2012. 35(8): p. 1716-1722.
- Harkness, E., et al., Identifying psychosocial interventions that improve both physical and mental health in patients with diabetes: a systematic review and meta-analysis. Diabetes Care, 2010. 33(4): p. 926-930.
- Yang, Q., et al., Art Therapy Alleviates the Levels of Depression and Blood Glucose in Diabetic Patients: A Systematic Review and Meta-Analysis. Frontiers in psychology, 2021. 12: p. 639626.
- Serlachius, A.S., et al., A randomized controlled trial of cognitive behaviour therapy to improve glycaemic control and psychosocial wellbeing in adolescents with type 1 diabetes. J Health Psychol, 2016. 21(6): p. 1157-1169.
- de Wit, M., et al., Monitoring and discussing health-related quality of life in adolescents with type 1 diabetes improve psychosocial well-being: a randomized controlled trial. Diabetes Care, 2008. 31(8): p. 1521-1526.
- Efthymiadis, A., M. Bourlaki, and A. Bastounis, The effectiveness of psychological interventions on mental health and quality of life in people living with type 1 diabetes: a systematic review and meta-analysis. Diabetology International, 2022.
- van der Feltz-Cornelis, C.M., et al., Effect of interventions for major depressive disorder and significant depressive symptoms in patients with diabetes mellitus: a systematic review and meta-analysis. Gen Hosp Psychiatry, 2010. 32(4): p. 380-395.
- Winkley, K., et al., Psychological interventions to improve glycaemic control in patients with type 1 diabetes: systematic review and meta-analysis of randomised controlled trials. BMJ, 2006. 333(7558): p. 65.
- Alam, R., et al., An updated meta-analysis to assess the effectiveness of psychological interventions delivered by psychological specialists and generalist clinicians on glycaemic control and on psychological status. Patient Educ Couns, 2009. 75(1): p. 25-36.
- Delamater, A.M., et al., Psychosocial therapies in diabetes: report of the Psychosocial Therapies Working Group. Diabetes Care, 2001. 24(7): p. 1286-1292.
- Mendez, F.J. and M. Belendez, Effects of a behavioral intervention on treatment adherence and stress management in adolescents with IDDM. Diabetes Care, 1997. 20(9): p. 1370-1375.
- Anderson, B.J., et al., Depressive symptoms and quality of life in adolescents with type 2 diabetes: baseline data from the TODAY study. Diabetes Care, 2011. 34(10): p. 2205-2207.
- Wilfley, D.E., L. Citrome, and B.K. Herman, Characteristics of binge eating disorder in relation to diagnostic criteria. Neuropsychiatric Disease & Treatment, 2016. 12: p. 2213-2223.
- Gabbs, M.H., et al., Poor sleep, increased stress and metabolic comorbidity in adolescents and youth with type 2 diabetes. Canadian Journal of Diabetes, 2022. 46(2): p. 142-149.
- Katz, L.L., et al., Correlates of Medication Adherence in the TODAY Cohort of Youth With Type 2 Diabetes. Diabetes care, 2016. 39(11): p. 1956-1962.
- McVoy, M., et al., Mental health comorbidity and youth onset type 2 diabetes: A systematic review of the literature. International journal of psychiatry in medicine, 2022: p. 912174211067335.
- Trief, P.M., et al., Diabetes distress in young adults with youth-onset type 2 diabetes: TODAY2 study results. Diabetes care, 2022. 45(3): p. 529-537.
- Katon, W., et al., Effect of depression and diabetes mellitus on the risk for dementia: a national population-based cohort study. JAMA Psychiatry, 2015. 72(6): p. 612-619.
- Limongi, F., et al., Prevalence of diabetes and depressive symptomatology and their effect on mortality risk in elderly Italians: the Italian Longitudinal Study on Aging. Diabetes & Metabolism, 2014. 40(5): p. 373-378.
- Sun, C., et al., Mobile Phone-Based Telemedicine Practice in Older Chinese Patients with Type 2 Diabetes Mellitus: Randomized Controlled Trial. JMIR Mhealth Uhealth, 2019. 7(1): p. e10664.
- Park, S.C., et al., Screening for depressive disorder in elderly patients with chronic physical diseases using the patient health questionnaire-9. Psychiatry Investigation, 2017. 14(3): p. 306-313.
- Chen, F., et al., Risk factors for depression in elderly diabetic patients and the effect of metformin on the condition. BMC public health, 2019. 19(1): p. 1063.
- Yap, J.M., et al., Effectiveness of technology-based psychosocial interventions on diabetes distress and health-relevant outcomes among type 2 diabetes mellitus: A systematic review and meta-analysis. Journal of telemedicine and telecare, 2021: p. 1357633X211058329.
- Kaveh, M.H., M.R. Faradonbeh, and S. Kaveh, Telehealth impact on biomedical, psychosocial, and behavioural outcomes in patients with diabetes older than 50 years: A systematic synthesis without meta-analysis. Journal of telemedicine and telecare, 2021: p. 1357633X211052222.
- Park, M. and C.F. Reynolds, Depression among older adults with diabetes mellitus. Clinics in Geriatric Medicine, 2015. 31(1): p. 117-137.
- Canadian Centre on Substance Abuse and Addiction. Available from: https://www.ccsa.ca/canadian-drug-trends.
- Canadian Tobacco and Nicotine Survey (CTNS): summary of results for 2020. Available from: https://www.canada.ca/en/health-canada/services/canadian-tobacco-nicotine-survey/2020-summary.html.
- zzz
- Knott, C., S. Bell, and A. Britton, Alcohol Consumption and the Risk of Type 2 Diabetes: A Systematic Review and Dose-Response Meta-analysis of More Than 1.9 Million Individuals From 38 Observational Studies. Diabetes Care, 2015. 38(9): p. 1804-1812.
- Tetzschner, R., K. Norgaard, and A. Ranjan, Effects of alcohol on plasma glucose and prevention of alcohol-induced hypoglycemia in type 1 diabetes-A systematic review with GRADE. Diabetes Metab Res Rev, 2018. 34(3).
- Pastor, A., et al., Glucose patterns following alcohol and illicit drug use in young adults with type 1 diabetes: A flash glucose monitoring study. Endocrinol Diabetes Metab, 2021. 4(3): p. e00257.
- Ahmed, A.T., A.J. Karter, and J. Liu, Alcohol consumption is inversely associated with adherence to diabetes self-care behaviours. Diabet Med, 2006. 23(7): p. 795-802.
- Maddatu, J., E. Anderson-Baucum, and C. Evans-Molina, Smoking and the risk of type 2 diabetes. Transl Res, 2017. 184: p. 101-107.
- Hu, Y., et al., Smoking Cessation, Weight Change, Type 2 Diabetes, and Mortality. N Engl J Med, 2018. 379(7): p. 623-632.
- Das, S.L., et al., Newly diagnosed diabetes mellitus after acute pancreatitis: a systematic review and meta-analysis. Gut, 2014. 63(5): p. 818-831.
- Huang, J., X. Wang, and Y. Zhang, Specific types of alcoholic beverage consumption and risk of type 2 diabetes: A systematic review and meta-analysis. J Diabetes Investig, 2017. 8(1): p. 56-68.
- Imtiaz, S. and J. Rehm, The relationship between cannabis use and diabetes: Results from the National Epidemiologic Survey on Alcohol and Related Conditions III. Drug Alcohol Rev, 2018. 37(7): p. 897-902.
- Rajavashisth, T.B., et al., Decreased prevalence of diabetes in marijuana users: cross-sectional data from the National Health and Nutrition Examination Survey (NHANES) III. BMJ Open, 2012. 2: p. e000494.
- Bancks, M.P., et al., Marijuana use and risk of prediabetes and diabetes by middle adulthood: the Coronary Artery Risk Development in Young Adults (CARDIA) study. Diabetologia, 2015. 58(12): p. 2736-2744.
- Danielsson, A.K., et al., Cannabis Use as Risk or Protection for Type 2 Diabetes: A Longitudinal Study of 18 000 Swedish Men and Women. J Diabetes Res, 2016. 2016: p. 6278709.
- Lin Li, e.a., Opioids and Risk of Type 2 Diabetes in Adults with Non-Cancer Pain. Pain Physician, 2013: p. 77-88.
- Fareed, A., et al., Predictors of diabetes mellitus and abnormal blood glucose in patients receiving opioid maintenance treatment. Am J Addict, 2013. 22(4): p. 411-416.
- Winhusen, T., et al., Medical complications associated with substance use disorders in patients with type 2 diabetes and hypertension: electronic health record findings. Addiction, 2019. 114(8): p. 1462-1470.
- Pan, A., et al., Relation of Smoking With Total Mortality and Cardiovascular Events Among Patients With Diabetes Mellitus: A Meta-Analysis and Systematic Review. Circulation, 2015. 132(19): p. 1795-1804.
- Koppes, L.L., et al., Meta-analysis of the relationship between alcohol consumption and coronary heart disease and mortality in type 2 diabetic patients. Diabetologia, 2006. 49(4): p. 648-652.
- Hirai, F.E., et al., Severe hypoglycemia and smoking in a long-term type 1 diabetic population: Wisconsin Epidemiologic Study of Diabetic Retinopathy. Diabetes Care, 2007. 30(6): p. 1437-1441.
- Jensen, M.H., et al., Smoking is Associated With Increased Risk of Not Achieving Glycemic Target, Increased Glycemic Variability, and Increased Risk of Hypoglycemia for People With Type 1 Diabetes. J Diabetes Sci Technol, 2021. 15(4): p. 827-832.
- Lohse, T., et al., Heavy Smoking Is More Strongly Associated with General Unhealthy Lifestyle than Obesity and Underweight. PLoS One, 2016. 11(2): p. e0148563.
- Stenstrom, U., Andersson, P. O. , Smoking, blood glucose control, and locus of control beliefs in people with type 1 diabetes mellitus. Diabetes research and clinical practice, 2000. 50(2): p. 103-107.
- Cooper, H., et al., Risk factors for recurrent admissions with diabetic ketoacidosis: a case-control observational study. Diabetic Medicine, 2016. 33(4): p. 523-528.
- Ravert, R.D., Alcohol management strategies of college students with diabetes. Patient Educ Couns, 2009. 77(1): p. 97-102.
- Lee, P., J.R. Greenfield, and L.V. Campbell, Managing young people with Type 1 diabetes in a 'rave' new world: metabolic complications of substance abuse in Type 1 diabetes. Diabet Med, 2009. 26(4): p. 328-333.
- Pancer, J. and K. Dasgupta, Effects of Cannabis Use in Youth and Young Adults With Type 1 Diabetes: The Highs, the Lows, the Don't Knows. Canadian journal of diabetes, 2020. 44(2): p. 121-127.
- Kinney, G.L., et al., Cannabis Use Is Associated With Increased Risk for Diabetic Ketoacidosis in Adults With Type 1 Diabetes: Findings From the T1D Exchange Clinic Registry. Diabetes Care, 2020. 43(1): p. 247-249.
- Lung, T.W., et al., A meta-analysis of the relative risk of mortality for type 1 diabetes patients compared to the general population: exploring temporal changes in relative mortality. PLoS One, 2014. 9(11): p. e113635.
- Gagnum, V., et al., Long-term Mortality and End-Stage Renal Disease in a Type 1 Diabetes Population Diagnosed at Age 15-29 Years in Norway. Diabetes Care, 2017. 40(1): p. 38-45.
- Feltbower, R.G., et al., Acute complications and drug misuse are important causes of death for children and young adults with type 1 diabetes: results from the Yorkshire Register of diabetes in children and young adults. Diabetes Care, 2008. 31(5): p. 922-926.
- Blomster, J.I., et al., The harms of smoking and benefits of smoking cessation in women compared with men with type 2 diabetes: an observational analysis of the ADVANCE (Action in Diabetes and Vascular Disease: Preterax and Diamicron modified release Controlled Evaluation) trial. BMJ Open, 2016. 6(1): p. e009668.
- Seet, R.C., et al., Acute effects of cigarette smoking on insulin resistance and arterial stiffness in young adults. Atherosclerosis, 2012. 224(1): p. 195-200.
- Al Sayah, F., et al., Diabetic Foot Disease, Self-Care and Clinical Monitoring in Adults with Type 2 Diabetes: The Alberta's Caring for Diabetes (ABCD) Cohort Study. Can J Diabetes, 2015. 39 Suppl 3: p. S120-S126.
- Rehm, J., et al., Dose-Response Relationships between Levels of Alcohol Use and Risks of Mortality or Disease, for All People, by Age, Sex, and Specific Risk Factors. Nutrients, 2021. 13(8).
- Rehm, J., et al., The relationship between different dimensions of alcohol use and the burden of disease-an update. Addiction, 2017. 112(6): p. 968-1001.
- Niskanen, L., et al., Excess mortality in Finnish diabetic subjects due to alcohol, accidents and suicide: a nationwide study. Eur J Endocrinol, 2018. 179(5): p. 299-306.
- Mehta, G. and A. Hirji, The Outcome of Structured Education in Adults With Type 2 Diabetes Mellitus and Substance Use Disorder: A Literature Review. Canadian journal of diabetes, 2020. 44(6): p. 487-493.
- Ng, B.P., et al., Opioid dispensing among adult Medicaid enrollees by diabetes status. Curr Med Res Opin, 2020. 36(10): p. 1577-1581.
- Kerr, E.A., et al., Beyond comorbidity counts: how do comorbidity type and severity influence diabetes patients' treatment priorities and self-management? J Gen Intern Med, 2007. 22(12): p. 1635-1640.
- Gautam S, F.L., Mikhail OI, Chan W, Turner BJ, Longitudinal Analysis of Opioid Analgesic Dose and Diabetes Quality of Care Measures. Pain Medicine, 2015. 16(11).
- Opioid use disorder and type 2 diabetes mellitus: effect of participation in buprenorphine-naloxone substitution programs on glycemic control Can Fam Physician, 2017. 63.
- Diabetes Canada. Quick Reference Guide: ABCDES of Diabetes Care. 2020. Available from: https://guidelines.diabetes.ca/fullguidelines/cpgrefguide.
- Wray, J.M., et al., A Meta-Analysis of Brief Tobacco Interventions for Use in Integrated Primary Care. Nicotine Tob Res, 2018. 20(12): p. 1418-1426.
- Nagrebetsky, A., et al., Smoking cessation in adults with diabetes: A systematic review and meta-analysis of data from randomised controlled trials. BMJ Open, 2014. 4 (3) (no pagination)(e004107).
- Russo, C., et al., Efficacy and Safety of Varenicline for Smoking Cessation in Patients With Type 2 Diabetes: A Randomized Clinical Trial. JAMA Netw Open, 2022. 5(6): p. e2217709.
- Bush, K.e.a., The AUDIT Alcohol Consumption Questions (AUDIT-C). ARCH INTERN MED, 1998. 158.
- Knox, J., et al., Prevention, screening, and treatment for heavy drinking and alcohol use disorder. The Lancet Psychiatry, 2019. 6(12): p. 1054-1067.
- al , R.S.E.e., Brief Alcohol Intervention Among At-Risk Drinkers with Diabetes. Substance Abuse: Research and Treatment, 2010. 4.
- Wisk, L.E., et al., Psychoeducational Messaging to Reduce Alcohol Use for College Students With Type 1 Diabetes: Internet-Delivered Pilot Trial. J Med Internet Res, 2021. 23(9): p. e26418.
- Giovannucci, E., et al., Diabetes and cancer: a consensus report. Diabetes Care, 2010. 33(7): p. 1674-1685.
- Bajaj, H.S., et al., Diabetes Canada Position Statement on Recreational Cannabis Use in Adults and Adolescents With Type 1 and Type 2 Diabetes. Can J Diabetes, 2019. 43(6): p. 372-376.
- Fischer, B., et al., Lower-Risk Cannabis Use Guidelines: A Comprehensive Update of Evidence and Recommendations. Am J Public Health, 2017. 107(8): p. e1-e12.
- Gates, P.J., et al., Psychosocial interventions for cannabis use disorder. Cochrane Database Syst Rev, 2016(5): p. CD005336.
- Klausen, M.K., et al., The role of glucagon-like peptide 1 (GLP-1) in addictive disorders. Br J Pharmacol, 2022. 179(4): p. 625-641.
- Sarkar, S. and Y.P.S. Balhara, Diabetes mellitus and suicide. Indian J Endocrinol Metab, 2014. 18(4): p. 468-474.
- Wang, B., et al., Suicide risk in patients with diabetes: A systematic review and meta-analysis. European Journal of Endocrinology, 2017. 177(4): p. R169-R181.
- Myers, A.K., et al., Brief report: depression and history of suicide attempts in adults with new-onset type 2 diabetes. Psychoneuroendocrinology, 2013. 38(11): p. 2810-2814.
- Fuller-Thomson, E., J.L. Milinovich, and J.R. Merighi, Lifetime prevalence of comorbid mood disorders in a representative sample of Canadians with type 1 diabetes. J Diabetes Complications, 2010. 24(5): p. 297-300.
- Hill, R.M., et al., Suicide Risk in Youth and Young Adults with Type 1 Diabetes: a Review of the Literature and Clinical Recommendations for Prevention. Curr Diab Rep, 2021. 21(12): p. 51.
- Barron, E., et al., Associations of type 1 and type 2 diabetes with COVID-19-related mortality in England: a whole-population study. The Lancet Diabetes & Endocrinology, 2020. 8(10): p. 813-822.
- Sathish, T., et al., Proportion of newly diagnosed diabetes in COVID-19 patients: A systematic review and meta-analysis. Diabetes Obes Metab, 2021. 23(3): p. 870-874.
- Diabetes Canada. Relationship between Diabetes and COVID-19. 2021. Available from: https://www.diabetes.ca/campaigns/covid-19-(coronavirus)-and-diabetes.
- Xie, Y. and Z. Al-Aly, Risks and burdens of incident diabetes in long COVID: a cohort study. The Lancet Diabetes & Endocrinology, 2022. 10(5): p. 311-321.
- Guo, W., et al., Diabetes is a risk factor for the progression and prognosis of COVID-19. Diabetes Metab Res Rev, 2020: p. e3319.
- Gallagher, M.W., et al., The Impact of Covid-19 Experiences and Associated Stress on Anxiety, Depression, and Functional Impairment in American Adults. Cognit Ther Res, 2020. 44(6): p. 1043-1051.
- Robinson, D., In for the long haul: persisting symptoms of COVID-19. Diabetes Communicator, 2022: p. 13-16.
- Aiyegbusi, O.L., et al., Symptoms, complications and management of long COVID: a review. J R Soc Med, 2021. 114(9): p. 428-442.
- Al-Aly, Z., B. Bowe, and Y. Xie, Long COVID after breakthrough SARS-CoV-2 infection. Nat Med, 2022. 28(7): p. 1461-1467.
- Agency, U.H.S., The effectiveness of vaccination against long COVID: A rapid evidence briefing. 2022.
- L'Italien GJ, C.D., Kan HJ, et al. , Comparison of metabolic syndrome incidence among schizophrenia patients treated with aripiprazole versus olanzapine or placebo. Journal of Clinical Psychiatry, 2007. 68(10).
- Canada, G.o. Post Covid-19 Condition (long COVID). 2019 June 12 2022]; Available from: https://www.canada.ca/en/public-health/services/ diseases/2019-novel-coronavirus-infection/symptoms/post-covid- 19-condition.html.
- Xie, Y., E. Xu, and Z. Al-Aly, Risks of mental health outcomes in people with covid-19: cohort study. BMJ, 2022. 376: p. e068993.
- Pignone, M.P., et al., Screening for depression in adults: a summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med, 2002. 136(10): p. 765-776.
- Ishizawa, K., et al., The relationship between depressive symptoms and diabetic complications in elderly patients with diabetes: Analysis using the Diabetes Study from the Center of Tokyo Women's Medical University (DIACET). Journal of Diabetes and its Complications, 2016. 30(4): p. 597-602.
- van Dooren, F.E.P., et al., Psychological and personality factors in type 2 diabetes mellitus, presenting the rationale and exploratory results from The Maastricht Study, a population-based cohort study. BMC psychiatry, 2016. 16: p. 17.
- Polonsky, W.H., et al., Assessment of diabetes-related distress. Diabetes Care, 1995. 18(6): p. 754-760.
- van Bastelaar, K.M., et al., Diabetes-specific emotional distress mediates the association between depressive symptoms and glycaemic control in type 1 and type 2 diabetes. Diabet Med, 2010. 27(7): p. 798-803.
- Furuya, M., et al., Comparative validity of the WHO-5 Well-Being Index and two-question instrument for screening depressive symptoms in patients with type 2 diabetes. Acta Diabetol, 2013. 50(2): p. 117-121.
- Collins, M.M., P. Corcoran, and I.J. Perry, Anxiety and depression symptoms in patients with diabetes. Diabet Med, 2009. 26(2): p. 153-161.
- Fisher, L., et al., A longitudinal study of affective and anxiety disorders, depressive affect and diabetes distress in adults with Type 2 diabetes. Diabet Med, 2008. 25(9): p. 1096-1101.
- Mantyselka, P., et al., Association of depressive symptoms with impaired glucose regulation, screen-detected, and previously known type 2 diabetes: findings from the Finnish D2D survey. Diabetes Care, 2011. 34(1): p. 71-76.
- Piatt, G.A., et al., 3-year follow-up of clinical and behavioral improvements following a multifaceted diabetes care intervention: results of a randomized controlled trial. Diabetes Educ, 2010. 36(2): p. 301-309.
- Bilgin, A., G. Muz, and G.E. Yuce, The effect of motivational interviewing on metabolic control and psychosocial variables in individuals diagnosed with diabetes: Systematic review and meta-analysis. Patient Educ Couns, 2022. 105(9): p. 2806-2823.
- Huang, C.Y., et al., Effects of motivational enhancement therapy plus cognitive behaviour therapy on depressive symptoms and health-related quality of life in adults with type II diabetes mellitus: a randomised controlled trial. Quality of Life Research, 2016. 25(5): p. 1275-1283.
- Li, C., et al., A systematic review and meta-analysis of randomized controlled trials of cognitive behavior therapy for patients with diabetes and depression. Journal of psychosomatic research, 2017. 95: p. 44-54.
- Ngan, H.Y., Y.Y. Chong, and W.T. Chien, Effects of mindfulness- and acceptance-based interventions on diabetes distress and glycaemic level in people with type 2 diabetes: Systematic review and meta-analysis. Diabetic medicine : a journal of the British Diabetic Association, 2021. 38(4): p. e14525.
- Maghsoudi, Z., et al., Efficacy Of Acceptance And Commitment Therapy For Emotional Distress In The Elderly With Type 2 Diabetes: A Randomized Controlled Trial. Diabetes Metab Syndr Obes, 2019. 12: p. 2137-2143.
- Sakamoto, R., et al., Efficacy of acceptance and commitment therapy for people with type 2 diabetes: Systematic review and meta-analysis. J Diabetes Investig, 2022. 13(2): p. 262-270.
- Davoudi, M., et al., Effectiveness of acceptance and commitment therapy (ACT) on depression and sleep quality in painful diabetic neuropathy: a randomized clinical trial. Journal of diabetes and metabolic disorders, 2020. 19(2): p. 1081-1088.
- Osborn, C.Y. and L.E. Egede, Validation of an Information-Motivation-Behavioral skills model of Diabetes Self-Care (IMB-DSC). Patient Educ Couns, 2010. 79(1): p. 49-54.
- Maindal, H.T., et al., Effect on motivation, perceived competence, and activation after participation in the ''Ready to Act'' programme for people with screen-detected dysglycaemia: a 1-year randomised controlled trial, Addition-DK. Scand J Public Health, 2011. 39(3): p. 262-271.
- Attari, A., et al., Effect of stress management training on glycemic control in patients with type 1 diabetes. Diabetes Res Clin Pract, 2006. 73(1): p. 23-28.
- Soo, H. and S. Lam, Stress management training in diabetes mellitus. J Health Psychol, 2009. 14(7): p. 933-943.
- Keogh, K.M., et al., Psychological family intervention for poorly controlled type 2 diabetes. Am J Manag Care, 2011. 17(2): p. 105-113.
- Wysocki, T., et al., Randomized trial of behavioral family systems therapy for diabetes: maintenance of effects on diabetes outcomes in adolescents. Diabetes Care, 2007. 30(3): p. 555-560.
- Wysocki, T., et al., Randomized, controlled trial of Behavioral Family Systems Therapy for Diabetes: maintenance and generalization of effects on parent-adolescent communication. Behav Ther, 2008. 39(1): p. 33-46.
- Armour, T.A., et al., The effectiveness of family interventions in people with diabetes mellitus: a systematic review. Diabet Med, 2005. 22(10): p. 1295-1305.
- Mathiesen, A.S., et al., Psychosocial interventions for reducing diabetes distress in vulnerable people with type 2 diabetes mellitus: a systematic review and meta-analysis. Diabetes Metab Syndr Obes, 2019. 12: p. 19-33.
- Schmidt, C.B., et al., Systematic review and meta-analysis of psychological interventions in people with diabetes and elevated diabetes-distress. Diabet Med, 2018.
- Cradock, K.A., et al., Behaviour change techniques targeting both diet and physical activity in type 2 diabetes: A systematic review and meta-analysis. International Journal of Behavioral Nutrition and Physical Activity, 2017. 14(1): p. 18.
- Chen, S.M., et al., Effects of motivational interviewing intervention on self-management, psychological and glycemic outcomes in type 2 diabetes: a randomized controlled trial. Int J Nurs Stud, 2012. 49(6): p. 637-644.
- Huang, Y., et al., Collaborative care for patients with depression and diabetes mellitus: a systematic review and meta-analysis. BMC Psychiatry, 2013. 13: p. 260.
- Atlantis, E., P. Fahey, and J. Foster, Collaborative care for comorbid depression and diabetes: a systematic review and meta-analysis. BMJ Open, 2014. 4(4): p. e004706.
- Petrak, F. and S. Herpertz, Treatment of depression in diabetes: an update. Curr Opin Psychiatry, 2009. 22(2): p. 211-217.
- Baumeister, H., N. Hutter, and J. Bengel, Psychological and pharmacological interventions for depression in patients with diabetes mellitus: an abridged Cochrane review. Diabetic Medicine, 2014. 31(7): p. 773-786.
- de Groot, M., et al., Can lifestyle interventions do more than reduce diabetes risk? Treating depression in adults with type 2 diabetes with exercise and cognitive behavioral therapy. Curr Diab Rep, 2012. 12(2): p. 157-166.
- Wang, M.Y., et al., A systematic review of the efficacy of non-pharmacological treatments for depression on glycaemic control in type 2 diabetics. J Clin Nurs, 2008. 17(19): p. 2524-2530.
- Chapman, A., et al., Psychological interventions for the management of glycemic and psychological outcomes of type 2 diabetes mellitus in china: a systematic review and meta-analyses of randomized controlled trials. Frontiers in Public Health, 2015. 3: p. 252.
- van Son, J., et al., The association between mindfulness and emotional distress in adults with diabetes: could mindfulness serve as a buffer? Results from Diabetes MILES: The Netherlands. Journal of Behavioral Medicine, 2015. 38(2): p. 251-260.
- Tovote, K.A., et al., Individual mindfulness-based cognitive therapy and cognitive behavior therapy for treating depressive symptoms in patients with diabetes: results of a randomized controlled trial. Diabetes Care, 2014. 37(9): p. 2427-2434.
- Hermanns, N., et al., The effect of a Diabetes-Specific Cognitive Behavioral Treatment Program (DIAMOS) for patients with diabetes and subclinical depression: results of a randomized controlled trial. Diabetes Care, 2015. 38(4): p. 551-560.
- Hessler, D., et al., Reductions in regimen distress are associated with improved management and glycemic control over time. Diabetes Care, 2014. 37(3): p. 617-624.
- Katon, W.J., et al., Collaborative care for patients with depression and chronic illnesses. N Engl J Med, 2010. 363(27): p. 2611-2620.
- Polonsky, W.H. and R.A. Jackson, What's so tough about taking insulin? Addressing the problem of psychological insulin resistance in type 2 diabetes. Clinical Diabetes, 2004. 22(3): p. 147.
- Barnard, K., et al., Fear of hypoglycaemia in parents of young children with type 1 diabetes: a systematic review. BMC Pediatr, 2010. 10: p. 50.
- Wild, D., et al., A critical review of the literature on fear of hypoglycemia in diabetes: implications for diabetes management and patient education. Patient Educ Couns, 2007. 68(1): p. 10-15.
- Ekong, G. and J. Kavookjian, Motivational interviewing and outcomes in adults with type 2 diabetes: a systematic review. Patient Educ Couns, 2016. 99(6): p. 944-952.
- Abidi, S., et al., D-WISE: Diabetes Web-Centric Information and Support Environment: conceptual specification and proposed evaluation. Can J Diabetes, 2014. 38(3): p. 205-211.
- Graves, H., et al., Psychological skills training to support diabetes self-management: qualitative assessment of nurses' experiences. Prim Care Diabetes, 2016. 10(5): p. 376-382.
- Fournier, M., D. De Ridder, and J. Bensing, Optimism and adaptation to chronic disease: The role of optimism in relation to self-care options of type 1 diabetes mellitus, rheumatoid arthritis and multiple sclerosis. Br J Health Psychol, 2002. 7(Part 4): p. 409-432.
- Seligman, M.E. and M. Csikszentmihalyi, Positive psychology. an introduction. Am Psychol, 2000. 55(1): p. 5-14.
- Varela-Moreno, E., et al., Effectiveness of eHealth-Based Psychological Interventions for Depression Treatment in Patients With Type 1 or Type 2 Diabetes Mellitus: A Systematic Review. Front Psychol, 2021. 12: p. 746217.
- Oyedeji, A.D., et al., Effectiveness of non-specialist delivered psychological interventions on glycemic control and mental health problems in individuals with type 2 diabetes: a systematic review and meta-analysis. Int J Ment Health Syst, 2022. 16(1): p. 9.
- Singh, V.P. and B. Khandelwal, Effect of Yoga and Exercise on Glycemic Control and Psychosocial Parameters in Type 2 Diabetes Mellitus: A Randomized Controlled Study. International journal of yoga, 2020. 13(2): p. 144-151.
- Xia, Z., J.W. DePierre, and L. Nassberger, Tricyclic antidepressants inhibit IL-6, IL-1 beta and TNF-alpha release in human blood monocytes and IL-2 and interferon-gamma in T cells. Immunopharmacology, 1996. 34(1): p. 27-37.
- Maes, M., et al., Negative immunoregulatory effects of antidepressants: inhibition of interferon-gamma and stimulation of interleukin-10 secretion. Neuropsychopharmacology, 1999. 20(4): p. 370-379.
- Kauffman, R.P., et al., Impact of the selective serotonin reuptake inhibitor citalopram on insulin sensitivity, leptin and basal cortisol secretion in depressed and non-depressed euglycemic women of reproductive age. Gynecol Endocrinol, 2005. 21(3): p. 129-137.
- Weber-Hamann, B., et al., Improved insulin sensitivity in 80 nondiabetic patients with MDD after clinical remission in a double-blind, randomized trial of amitriptyline and paroxetine. J Clin Psychiatry, 2006. 67(12): p. 1856-1861.
- Stahl, S., The prescriber's guide. 6th ed. 2017, New York, NY: Cambridge University Press.
- Andersohn F, Schade R, and e.a. Suissa S, Long-Term Use of Antidepressants for Depressive Disorders and the Risk of Diabetes Mellitus. American Journal of Psychiatry, 2009. 166: p. 591-598.
- Mumoli, N., et al., Diabetes mellitus associated with clomipramine treatment: a retrospective analysis. Acta Diabetol, 2014. 51(1): p. 167-168.
- Gagnon, J., et al., The Impact of Antidepressant Therapy on Glycemic Control in Canadian Primary Care Patients With Diabetes Mellitus. Front Nutr, 2018. 5: p. 47.
- Auclair, A.L., et al., Levomilnacipran (F2695), a norepinephrine-preferring SNRI: profile in vitro and in models of depression and anxiety. Neuropharmacology, 2013. 70: p. 338-347.
- Hall, J.A., et al., Safety and tolerability of duloxetine in the acute management of diabetic peripheral neuropathic pain: analysis of pooled data from three placebo-controlled clinical trials. Expert opinion on drug safety, 2010. 9(4): p. 525-537.
- Fagiolini, A., et al., Metabolic syndrome in bipolar disorder: findings from the Bipolar Disorder Center for Pennsylvanians. Bipolar Disord, 2005. 7(5): p. 424-430.
- Deuschle, M., Effects of antidepressants on glucose metabolism and diabetes mellitus type 2 in adults. Current opinion in psychiatry, 2013. 26(1): p. 60-65.
- Ma, Y., et al., Relations of depressive symptoms and antidepressant use to body mass index and selected biomarkers for diabetes and cardiovascular disease. American journal of public health, 2013. 103(8): p. e34-e43.
- Kivimaki, M., et al., Antidepressant medication use, weight gain, and risk of type 2 diabetes: a population-based study. Diabetes Care, 2010. 33(12): p. 2611-2616.
- Burcu, M., et al., Association of Antidepressant Medications With Incident Type 2 Diabetes Among Medicaid-Insured Youths. JAMA Pediatr, 2017. 171(12): p. 1200-1207.
- Kivimaki, M., et al., Antidepressant medication use and risk of hyperglycemia and diabetes mellitus: a noncausal association? Biol Psychiatry, 2011. 70(10): p. 978-984.
- Khapre, M., et al., Antidepressant use and glycemic control in diabetic population: A meta-analysis. Indian Journal of Endocrinology and Metabolism, 2020. 24(4): p. 295-300.
- Lopez-Yarto, M., et al., Do psychiatric medications, especially antidepressants, adversely impact maternal metabolic outcomes? J Affect Disord, 2012. 141(2-3): p. 120-129.
- Roopan, S. and E.R. Larsen, Use of antidepressants in patients with depression and comorbid diabetes mellitus: a systematic review. Acta neuropsychiatrica, 2017. 29(3): p. 127-139.
- Meng, H., J. Lu, and X. Zhang, Metabolic Influences of commonly used antidepressants on blood glucose homeostasis. Indian Journal of Pharmaceutical Sciences, 2019. 81(2): p. 188-189.
- Barnard, K., R.C. Peveler, and R.I. Holt, Antidepressant medication as a risk factor for type 2 diabetes and impaired glucose regulation: systematic review. Diabetes care, 2013. 36(10): p. 3337-3345.
- Woo, Y.S., et al., Association of treatment response with obesity and other metabolic risk factors in adults with depressive disorders: Results from a National Depression Cohort study in Korea (the CRESCEND study). Journal of Affective Disorders, 2016. 203: p. 190-198.
- Correll, C.U., et al., Effects of antipsychotics, antidepressants and mood stabilizers on risk for physical diseases in people with schizophrenia, depression and bipolar disorder. World Psychiatry, 2015. 14(2): p. 119-136.
- Erden, A., et al., Lithium intoxication and nephrogenic diabetes insipidus: a case report and review of literature. International journal of general medicine, 2013: p. 535-539.
- Vestergaard P, S.M., Does long-term lithium treatment induce diabetes mellitus? Neuropsychobiology, 1987. 17(3): p. 130-132.
- Nestsiarovich, A., et al., Diabetes mellitus risk for 102 drugs and drug combinations used in patients with bipolar disorder. Psychoneuroendocrinology, 2020. 112: p. 104511.
- Mittal, K., et al., A comprehensive analysis of mitochondrial genes variants and their association with antipsychotic-induced weight gain. Schizophr Res, 2017. 187: p. 67-73.
- Salvi, V., C. Mencacci, and F. Barone-Adesi, H1-histamine receptor affinity predicts weight gain with antidepressants. Eur Neuropsychopharmacol, 2016. 26(10): p. 1673-1677.
- Zhang, J.P., et al., Pharmacogenetic Associations of Antipsychotic Drug-Related Weight Gain: A Systematic Review and Meta-analysis. Schizophr Bull, 2016. 42(6): p. 1418-1437.
- Belcastro, V., et al., Metabolic and endocrine effects of valproic acid chronic treatment. Epilepsy Res, 2013. 107(1-2): p. 1-8.
- Vancampfort, D., et al., The impact of pharmacological and non-pharmacological interventions to improve physical health outcomes in people with schizophrenia: a meta-review of meta-analyses of randomized controlled trials. World Psychiatry, 2019. 18(1): p. 53-66.
- Maayan, L., J. Vakhrusheva, and C.U. Correll, Effectiveness of medications used to attenuate antipsychotic-related weight gain and metabolic abnormalities: a systematic review and meta-analysis. Neuropsychopharmacology, 2010. 35(7): p. 1520-1530.
- Holt, R.I.G.M., AJ., Association Between Antipsychotic Medication Use and Diabetes. Curr Diab Rep, 2019. 19(10): p. 96.
- Smith, M., et al., First-v. second-generation antipsychotics and risk for diabetes in schizophrenia: systematic review and meta-analysis. The British Journal of Psychiatry, 2008. 192(6): p. 406-411.
- Hartling, L., et al., Antipsychotics in Adults With Schizophrenia: ComparativeEffectiveness of First-Generation Versus Second-GenerationMedications. Annals of Internal Medicine, 2012.
- Heinonen, E., et al., Antipsychotic Use During Pregnancy and Risk for Gestational Diabetes: A National Register-Based Cohort Study in Sweden. CNS Drugs, 2022.
- Galbally, M., et al., The association between gestational diabetes mellitus, antipsychotics and severe mental illness in pregnancy: A multicentre study. The Australian & New Zealand journal of obstetrics & gynaecology, 2020. 60(1): p. 63-69.
- Fiedorowicz, J.G., et al., Systematic Review and Meta-analysis of Pharmacological Interventions for Weight Gain from Antipsychotics and Mood Stabilizers. Curr Psychiatry Rev, 2012. 8(1): p. 25-36.
- Yood, M.U., et al., The incidence of diabetes in atypical antipsychotic users differs according to agent--results from a multisite epidemiologic study. Pharmacoepidemiol Drug Saf, 2009. 18(9): p. 791-799.
- Deng, C., Effects of antipsychotic medications on appetite, weight, and insulin resistance. Endocrinol Metab Clin North Am 2013. 42(3): p. 545-563.
- Ballon, J.S., et al., Molecular pathophysiology of metabolic effects of antipsychotic medications. Trends Endocrinol Metab, 2014. 25(11): p. 593-600.
- Weston-Green, K., Xu-Feng Huang, and Chao Deng, Second generation antipsychotic-induced type 2 diabetes: a role for the muscarinic M3 receptor. CNS drugs, 2013.
- Crilly, J., The history of clozapine and its emergence in the US market: a review and analysis. Hist Psychiatry, 2007. 18(1): p. 39-60.
- Amato, D., Serotonin in antipsychotic drugs action. Behav Brain Res, 2015. 277: p. 125-135.
- American Diabetes Association; American Psychiatric Association, American Association of Clinical Endocrinologists, and North American Association for the Study of Obesity, Consensus development conference on antipsychotic drugs and obesity and diabetes. Diabetes Care, 2004. 27(2): p. 596-601.
- Kahn, R.S., et al., Effectiveness of antipsychotic drugs in first-episode schizophrenia and schizophreniform disorder: an open randomised clinical trial. Lancet, 2008. 371(9618): p. 1085-1097.
- Citrome, L., et al., Weight gain and changes in metabolic variables following olanzapine treatment in schizophrenia and bipolar disorder. Clinical drug investigation, 2011. 31: p. 455-482.
- Lord, C.C., et al., The atypical antipsychotic olanzapine causes weight gain by targeting serotonin receptor 2C. The Journal of clinical investigation, 2017. 127(9): p. 3402-3406.
- He, M., et al., Hypothalamic histamine H1 receptor-AMPK signaling time-dependently mediates olanzapine-induced hyperphagia and weight gain in female rats. Psychoneuroendocrinology, 2014. 42: p. 153-164.
- Davey, K.J., et al., Antipsychotics and the gut microbiome: olanzapine-induced metabolic dysfunction is attenuated by antibiotic administration in the rat. Transl Psychiatry, 2013. 3(10): p. e309.
- Coccurello, R., et al., 30 days of continuous olanzapine infusion determines energy imbalance, glucose intolerance, insulin resistance, and dyslipidemia in mice. J Clin Psychopharmacol, 2009. 29(6): p. 576-583.
- Chen, J., et al., Molecular Mechanisms of Antipsychotic Drug-Induced Diabetes. Front Neurosci, 2017. 11: p. 643.
- Weston-Green, K., Xu-Feng Huang, and Chao Deng, Second generation antipsychotic-induced type 2 diabetes: a role for the muscarinic M3 receptor. CNS Drugs, 2013. 27(12).
- Liu, M.-Z., et al., Drug-induced hyperglycaemia and diabetes: pharmacogenomics perspectives. Archives of pharmacal research, 2018. 41: p. 725-736.
- Bak, M., et al., Almost all antipsychotics result in weight gain: a meta-analysis. PLoS One, 2014. 9(4): p. e94112.
- Huhn, M., et al., Comparative efficacy and tolerability of 32 oral antipsychotics for the acute treatment of adults with multi-episode schizophrenia: a systematic review and network meta-analysis. The Lancet, 2019. 394(10202): p. 939-951.
- Woo, V., S.B. Harris, and R.L. Houlden, Canadian Diabetes Association position paper: Antipsychotic medications and associated risks of weight gain and diabetes. Canadian Journal of Diabetes, 2005. 29(2): p. 111-112.
- De Hert, M.e.a., Physical illness in patients with severe mental disorders. I. Prevalence, impact of medications and disparities in health care. World Psychiatry, 2011. 10(1).
- De Hert, M., et al., Metabolic and cardiovascular adverse effects associated with antipsychotic drugs. Nat Rev Endocrinol, 2011. 8(2): p. 114-126.
- Pillinger T, M.R., Vano L, et al, Comparative effects of 18 antipsychotics on metabolic function in patients with schizophrenia, predictors of metabolic dysregulation, and association with psychopathology: a systematic review and network meta-analysis. Lancet Psychiatry 2020. 7(1).
- Siafis, S., et al., Antipsychotic drugs: from receptor-binding profiles to metabolic side effects. Current neuropharmacology, 2018. 16(8): p. 1210-1223.
- Blonde L, K.H., Gutterman EM, L'Italien GJ, Kim MS, Hanssens L, McQuade RD. , Predicted risk of diabetes and coronary heart disease in patients with schizophrenia: aripiprazole versus standard of care. J Clin Psychiatry. , 2008. 69(5): p. 741-748.
- Citrome L, K.I., Baker RA, et al. , A review of real-world data on the effects of aripiprazole on weight and metabolic outcomes in adults. Curr Med Res Opin, 2014. 30(8).
- Zhang, Y., et al., The metabolic side effects of 12 antipsychotic drugs used for the treatment of schizophrenia on glucose: A network meta-analysis. BMC Psychiatry, 2017. 17(1): p. 373.
- Bernardo, M., et al., Real-World Data on the Adverse Metabolic Effects of Second-Generation Antipsychotics and Their Potential Determinants in Adult Patients: A Systematic Review of Population-Based Studies. Adv Ther, 2021. 38(5): p. 2491-2512.
- Ijaz, S., et al., Antipsychotic polypharmacy and metabolic syndrome in schizophrenia: a review of systematic reviews. BMC Psychiatry, 2018. 18(1): p. 275.
- Fraguas D, C.C., Merchan-Naranjo J, et al. , Efficacy and safety of second-generation antipsychotics in children and adolescents with psychotic and bipolar spectrum disorders: Comprehensive review of prospective head-to-head and placebo-controlled comparisons. Eur Neuropsychopharmacol 2011. 21.
- Newcomer, J.W., et al., Changes in metabolic parameters and body weight in brexpiprazole-treated patients with acute schizophrenia: pooled analyses of phase 3 clinical studies. Curr Med Res Opin, 2018. 34(12): p. 2197-2205.
- Forbes, A., et al., A Long-Term, Open-Label Study to Evaluate the Safety and Tolerability of Brexpiprazole as Maintenance Treatment in Adults with Schizophrenia. Int J Neuropsychopharmacol, 2018. 21(5): p. 433-441.
- Weiss, C., et al., The effects of brexpiprazole and aripiprazole on body weight as monotherapy in patients with schizophrenia and as adjunctive treatment in patients with major depressive disorder: an analysis of short-term and long-term studies. Int Clin Psychopharmacol, 2018. 33(5): p. 255-260.
- Corponi F, F.C., Bitter I, et al. , Novel antipsychotics specificity profile: A clinically oriented review of lurasidone, brexpiprazole, cariprazine and lumateperone. European Neuropsychopharmacology 2019. 29.
- Hobart M, Z.P., Skuban A, et al. , Long-Term, Open-Label Study to Evaluate the Safety and Tolerability of Brexpiprazole as Adjunctive Therapy in Adults With Major Depressive Disorder. J Clin Psychopharmacol, 2019. 39(3).
- Lao KSJ, H.Y., Wong ICK, et al. , Tolerability and Safety Profile of Cariprazine in Treating Psychotic Disorders, Bipolar Disorder and Major Depressive Disorder: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. CNS Drugs 2016. 30.
- Earley, W.R., et al., Efficacy and safety of cariprazine in bipolar I depression: A double-blind, placebo-controlled phase 3 study. Bipolar Disorders, 2020. 22(4): p. 372-384.
- Alvarez-Jimenez M, G.-B.C., Crespo-Facorro B, et al. , Antipsychotic-induced weight gain in chronic and first-episode psychotic disorders. CNS drugs, 2008. 22(7).
- Davies MJ, A.V., Collins BS, Gabbay RA, Green J, Maruthur NM, Rosas SE, Del Prato S, Mathieu C, Mingrone G, Rossing P, Tankova T, Tsapas A, Buse JB, Management of Hyperglycemia in Type 2 Diabetes, 2022. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care, 2022.
- Blonde, L., et al., American Association of Clinical Endocrinology Clinical Practice Guideline: Developing a Diabetes Mellitus Comprehensive Care Plan-2022 Update. Endocr Pract, 2022. 28(10): p. 923-1049.
- Samaras K, C.C., Mitchell AJ et al, Diabetes risk potentially underestimated in youth and children receiving antipsychotics. JAMA Psychiatry 2014. 71.
- Bobo WV, C.W., Stein CM et al. , Antipsychotics and the risk of type 2 diabetes mellitus in children and youth. JAMA Psychiatry 2013. 70.
- Nielsen, R.E., et al., Risk of diabetes in children and adolescents exposed to antipsychotics: a nationwide 12-year case-control study. J Am Acad Child Adolesc Psychiatry, 2014. 53(9): p. 971-979.e6.
- Jarskog, L.F., et al., Metformin for weight loss and metabolic control in overweight outpatients with schizophrenia and schizoaffective disorder. Am J Psychiatry, 2013. 170(9): p. 1032-1040.
- Galling B, R.A., Nielsen RE, et al. , Type 2 Diabetes Mellitus in Youth Exposed to Antipsychotics A Systematic Review and Meta-analysis. JAMA Psychiatry, 2016. 73(3).
- Correll CU, P.J., Parikh UH, et al. , Recognizing and monitoring adverse events of second-generation antipsychotics in children and adolescents. Child Adolesc Psychiatr Clinics North America, 2006. 15.
- De Hert, M. and J. Detraux, The Urgent Need for Optimal Monitoring of Metabolic Adverse Effects in Children and Youngsters Who Take On-label or Off-label Antipsychotic Medication. JAMA Psychiatry, 2018. 75(8): p. 771-772.
- Correll, C.U. and B. Galling, Polypharmacy in Youth Treated With Antipsychotics: Do Antidepressants or Stimulants Add to the Risk for Type 2 Diabetes? Journal of the American Academy of Child and Adolescent Psychiatry, 2017. 56(8): p. 634-635.
- Panagiotopoulos, C., R. Ronsley, and J. Davidson, Increased prevalence of obesity and glucose intolerance in youth treated with second-generation antipsychotic medications. Canadian Journal of Psychiatry, 2009. 54(11): p. 743-749.
- Rubin, D.M., et al., Risk for incident diabetes mellitus following initiation of second-generation antipsychotics among Medicaid-enrolled youths. JAMA Pediatr, 2015. 169(4): p. e150285.
- Stroup, T.S., et al., Effectiveness of olanzapine, quetiapine, risperidone, and ziprasidone in patients with chronic schizophrenia following discontinuation of a previous atypical antipsychotic. Am J Psychiatry, 2006. 163(4): p. 611-622.
- Stroup, T.S., et al., A randomized trial examining the effectiveness of switching from olanzapine, quetiapine, or risperidone to aripiprazole to reduce metabolic risk: Comparison of Antipsychotics for Metabolic Problems (CAMP). Am J Psychiatry, 2011. 168(9): p. 947-956.
- Procyshyn, R.M., Clinical handbook of psychotropic drugs. 22nd ed. 2017, Toronto: Hogrefe Publishing.
- Caemmerer, J., C.U. Correll, and L. Maayan, Acute and maintenance effects of non-pharmacologic interventions for antipsychotic associated weight gain and metabolic abnormalities: a meta-analytic comparison of randomized controlled trials. Schizophr Res, 2012. 140(1-3): p. 159-168.
- Reynolds, G.P., Pharmacogenetic Aspects of Antipsychotic Drug-induced Weight Gain - A Critical Review. Clinical Psychopharmacology and Neuroscience, 2012. 10(2).
- Lopresti, A.L., and Peter D. Drummond, Obesity and psychiatric disorders: commonalities in dysregulated biological pathways and their implications for treatment. Progress in Neuro-Psychopharmacology and Biological Psychiatry, 2013. 45.
- Reynolds, G.P. and S.L. Kirk, Metabolic side effects of antipsychotic drug treatment-pharmacological mechanisms. Pharmacology & therapeutics, 2010. 125(1): p. 169-179.
- Serretti, A., Laura Mandelli, and M. Laura, Antidepressants and body weight: a comprehensive review and meta-analysis. The Journal of clinical psychiatry 2010. 71(10).
- Reynolds GP, M.O., Mechanisms underlying metabolic disturbances associated with psychosis and antipsychotic drug treatment. J Psychopharmacol, 2017. 31(11).
- Peters, T., et al., The Role of Genetic Variation of BMI, Body Composition, and Fat Distribution for Mental Traits and Disorders: A Look-Up and Mendelian Randomization Study. Front Genet, 2020. 11: p. 373.
- Das C, M.G., Jagasia S et al, Second-generation antipsychotic use in schizophrenia and associated weight gain: a critical review and meta-analysis of behavioral and pharmacologic treatments. Ann Clin Psychiatry 2012. 24.
- Walker ER, M.R., Druss BG, Mortality in mental disorders and global disease burden implications: a systematic review and meta-analysis. JAMA Psychiatry 2015. 72(4).
- Chen WY, H.S., Chang CK, et al, Excess mortality and risk factors for mortality among patients with severe mental disorders receiving home care case management. Nord J Psychiatry 2020.
- Roedevand L, S.N., Elvsashagen T, et al, Cardiovascular risk remains high in schizophrenia with modest improvements in bipolar disorder during past decade. Acta Psychiatrica Scandinavica, 2019. 139(4).
- Ungar, T., S. Goldman, and M. Marcus, Reversed Shared Care in Mental Health: Bringing Primary Physical Health Care to Psychiatric Patients. Canadian Journal of Community Mental Health, 2013. 32(3): p. 1-16.
- Vancampfort, D., et al., Prevalence and predictors of type 2 diabetes mellitus in people with bipolar disorder: a systematic review and meta-analysis. J Clin Psychiatry, 2015. 76(11): p. 1490-1499.
- Gardner-Sood, P., et al., Cardiovascular risk factors and metabolic syndrome in people with established psychotic illnesses: baseline data from the IMPaCT randomized controlled trial. Psychological Medicine, 2015. 45(12): p. 2619-2629.
- Meyer, J., Medical illness and schizophrenia. 2nd ed. 2009, Arlington, VA: American Psychiatric Publishing, Inc.
- Smith, R.S., The macrophage theory of depression. Med Hypotheses, 1991. 35(4): p. 298-306.
- Fernandez-Real, J.M. and J.C. Pickup, Innate immunity, insulin resistance and type 2 diabetes. Trends Endocrinol Metab, 2008. 19(1): p. 10-16.
- Lambert, T.J., L.H. Chapman, and Consensus Working Group, Diabetes, psychotic disorders and antipsychotic therapy: a consensus statement. Med J Aust, 2004. 181(10): p. 544-548.
- Steylen, P.M., et al., Glycosylated hemoglobin as a screening test for hyperglycemia in antipsychotic-treated patients: a follow-up study. Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy, 2015. 8: p. 57-63.
- Hasnain M, Vieweg WV, Hollett B. Weight gain and glucose dysregulation with second-generation antipsychotics and antidepressants: a review for primary care physicians. Postgrad Med 2012;Jul;124(4):154-67. doi: 10.3810/pgm.2012.07.2577.
- Perez-Iglesias, R., et al., Course of weight gain and metabolic abnormalities in first treated episode of psychosis: the first year is a critical period for development of cardiovascular risk factors. International Journal of Neuropsychopharmacology, 2014. 17(1): p. 41-51.
- Group, T.S., et al., Binge eating, mood, and quality of life in youth with type 2 diabetes: baseline data from the today study. Diabetes Care, 2011. 34(4): p. 858-860.
- Adriaanse, M.C., et al., Diabetes-related symptoms and negative mood in participants of a targeted population-screening program for type 2 diabetes: The Hoorn Screening Study. Quality of Life Research, 2005. 14: p. 1501-1509.
- Smedslund, G., et al., Motivational interviewing for substance abuse. Campbell Systematic Reviews, 2011. 7(1): p. 1-126.
- Engler, P.A., S.E. Ramsey, and R.J. Smith, Alcohol use of diabetes patients: the need for assessment and intervention. Acta Diabetol, 2013. 50(2): p. 93-99.
- Ismail, K., K. Winkley, and S. Rabe-Hesketh, Systematic review and meta-analysis of randomised controlled trials of psychological interventions to improve glycaemic control in patients with type 2 diabetes. Lancet, 2004. 363(9421): p. 1589-1597.
- Grey, M., et al., Short-term effects of coping skills training as adjunct to intensive therapy in adolescents. Diabetes Care, 1998. 21(6): p. 902-908.
- Ellis, D.A., et al., The Effects of Multisystemic Therapy on Diabetes Stress Among Adolescents With Chronically Poorly Controlled Type 1 Diabetes: Findings From a Randomized, Controlled Trial. Pediatrics, 2005. 116(6): p. e826.
Diabetes Canada is the registered owner of all content on guidelines.diabetes.ca and ShopDC. For questions, please email info@diabetes.ca