Chapter Headings
Key Messages
- Heart failure is still under-recognized and misdiagnosed. This has significant clinical implications as the prognosis of untreated or undertreated heart failure is poor, and yet very effective proven therapies are widely available to most.
- Diabetes can cause heart failure independently of ischemic heart disease by causing a diabetic cardiomyopathy that may manifest in the setting of normal or reduced left ventricular ejection fraction. The incidence of heart failure is 2- to 4-fold higher in people with diabetes compared to those without and, when present, occurs at an earlier age.
- Even though heart failure in people with diabetes should be treated similarly to heart failure in those without diabetes, they are less likely to receive appropriate therapies. The presence of diabetes should not affect the decision for treatment of heart failure.
- Comorbidities, such as renal dysfunction and propensity for hyperkalemia, are more prevalent in people with diabetes and may influence heart failure drug doses and monitoring of therapy but not therapeutic targets.
Key Messages for People with Diabetes
- Heart failure is a type of heart disease in which the heart no longer pumps sufficient blood to meet the body's needs. Diabetes is a risk factor for heart failure.
- Symptoms of heart failure include shortness of breath, persistent coughing, fatigue, chest pain, weight gain or swelling of the feet, ankles and legs.
- A number of effective drug treatments are available to keep heart failure in check. Your health-care provider will discuss these with you.
- Certain glucose-lowering medications have the potential to worsen or help heart failure. If you have heart failure, this will influence which glucose-lowering medications your health-care provider selects for you.
Introduction
Type 2 diabetes often occurs in association with other cardiovascular (CV) risk factors, such as hypertension, dyslipidemia, smoking and obesity, which, together, are strongly associated with atherosclerosis, ischemic heart disease and left ventricular (LV) dysfunction (1). LV dysfunction can be clinically silent or associated with the typical clinical signs and symptoms of heart failure (e.g. peripheral edema, shortness of breath, fatigue), although the elderly may have atypical symptoms (2). These symptoms need to be differentiated from other conditions that may have similar presentations, such as chronic obstructive pulmonary disease, pneumonia, anemia, varicose veins, depression, etc.
Heart Failure in People with Diabetes
The diagnosis of heart failure is made by association of typical clinical signs and symptoms with objective evidence, such as that obtained from a chest x-ray, an echocardiogram or plasma natriuretic peptide testing (brain natriuretic peptide [BNP] and pro-hormone of BNP [NT-pro-BNP]) (2). Documentation of systolic and diastolic myocardial function is recommended at the time of diagnosis of heart failure or with any significant change in clinical stability. Heart failure can occur over the entire range of left ventricular ejection fractions (LVEF), from <10% to >60%. The measurement of plasma BNP and NT-pro-BNP, which are acutely released by ventricular myocytes when the myocardium is stretched due to increased filling pressures, may help make an accurate diagnosis where clinical uncertainty exists (3). However, the practicing health-care provider may still under-recognize and misdiagnose heart failure. This has significant clinical implications as the prognosis of untreated or undertreated heart failure is poor, yet very effective proven therapies are widely available. Because of this, many studies have explored the clinical utility of screening people with diabetes for the presence of reduced LV function with BNP/NT-pro- BNP testing. The results to date are mixed, with no clear consensus to institute this strategy. A recent analysis of the Action in Diabetes and Vascular disease: PreterAx and Diamicron MR Controlled Evaluation (ADVANCE) study assessed a number of biomarkers, including high sensitive C-reactive protein (hs-CRP), highly sensitive troponin T (hs-TnT) assay and interleukin 6. In a cohort of 3,098 participants in the ADVANCE study who underwent a nested case-cohort study, only NT-pro-BNP strongly and consistently improved the prediction of heart failure (4).
Diabetes is associated with increased prevalence of heart failure, both systolic (commonly defined as LVEF <40% or heart failure with a reduced ejection fraction) and diastolic (commonly defined as LVEF >50%, but also referred to as preserved systolic function or heart failure with preserved EF). However, the overlap between heart failure with preserved EF and reduced EF is considerable, and many people have a combination of systolic and diastolic dysfunction, although one is often reported to be predominant. Current tests, such as echocardiography, do usually fully characterize all aspects of systolic and diastolic dysfunction in individuals.
It is recognized that diabetes can cause heart failure independently of ischemic heart disease by causing a diabetic cardiomyopathy (5). Epidemiological studies have shown that the incidence of heart failure is 2- to 4-fold higher in people with diabetes compared to those without diabetes (6,7). Additionally, studies have shown the occurrence of asymptomatic abnormalities of ventricular systolic and diastolic function, independently from ischemic heart disease or systemic hypertension. While an increase in glycated hemoglobin (A1C) among individuals with diabetes is a recognized risk factor for heart failure (8–12), no prospective study to date has demonstrated that improved glycemic control significantly reduces the incidence of heart failure (13). Albuminuria is also an independent risk factor for heart failure, especially in people with diabetes. In individuals with and without diabetes, an increasing urinary albumin to creatinine ratio (ACR) is associated with a stepwise increase (2- to 4-fold) in the risk of heart failure development (10,14). Blockade of the renin angiotensin aldosterone system (RAAS) has been shown in large clinical trials of participants with cardiovascular disease (CVD) or diabetes to lower the risk of new-onset heart failure (15–17).
Treatment of Individuals with Both Diabetes and Heart Failure
In nearly every clinical trial involving people with heart failure, diabetes is present in over one-third of subjects. In the large landmark clinical trials of heart failure, subgroup analysis of populations with diabetes has shown that, despite their increased risk of morbidity and mortality, they derive greater absolute benefit from efficacious therapies as compared to people without diabetes (17–19). This was again demonstrated in the Prospective Comparison of ARNI with ACEI to Determine Impact on Global Mortality and Morbidity in Heart Failure (PARADIGM-HF) trial in which 8,442 participants with class II, III or IV heart failure and an EF of ≤40% were randomized to receive either LCZ696 (sacubitril/valsartan at a dose of 200 mg twice daily) or enalapril (at a dose of 10 mg twice daily), in addition to routine heart failure therapy. The primary outcome was a composite of death from CV causes or hospitalization for heart failure. LCZ696 was superior to enalapril in reducing the risks of death and of hospitalization for heart failure (p<0.001) (20). An analysis of 4,013 participants in the trial who had a diagnosis of diabetes based on A1C or prior history demonstrated that LCZ696 remained similarly efficacious, regardless of glycemic status (21). A similar finding was observed with the Systolic Heart failure treatment with the I
Therapeutic Considerations for Individuals with Both Diabetes and Heart Failure
People with diabetes are at increased risk for development of hyperkalemia and worsening renal dysfunction in the setting of RAAS blocking agents (24–29). Clinicians should be aware of this potential complication, especially in view of current guidelines advocating the expanded use of combined RAAS blockade in people with mild-to-moderate heart failure and low EF.
Three beta blockers have been shown to reduce morbidity and mortality for people with heart failure, reduced EF and diabetes: carvedilol, bisoprolol and metoprolol succinate. While overall glycemic control generally improves as heart failure is treated with evidence-based therapies, (30–32), carvedilol, in comparison to other beta blockers, has been shown to specifically improve glycemic control (19,33). For this reason, some clinicians prefer carvedilol as the beta blocker of choice in people with diabetes and heart failure. While there is a theoretical concern for the occurrence of severe hypoglycemia without awareness associated with the use of nonselective beta blockers, this has not been reported in clinical trials.
Numerous registries and reports indicate that persons with diabetes are less likely than those without diabetes to receive efficacious and evidence-based therapies for systolic heart failure. Perhaps this is due, in part, to the increased incidence of side effects and/or intolerance to RAAS blockade and the increased prevalence of renal disease in people with diabetes. However, even when controlled for these conditions, the differences persist. This is particularly concerning considering the increased absolute benefit the agents confer to people with heart failure and diabetes in comparison to unselected heart failure populations. As such, health-care prescribers must be diligent in providing these therapies.
Antihyperglycemic Agents and Heart Failure
Despite substantial understanding of the impact of antihyperglycemic therapy upon glucose control and microvascular disease, the heart failure specific response to intensive glycemic control and the various antihyperglycemic agents (discussed below) remains poorly understood (34).
Metformin
Metformin is an effective noninsulin antihyperglycemic agent but, based on isolated case reports and a biochemical rationale for a risk of lactic acidosis, it is approved for use under a warning in the setting of several conditions, including heart failure. Meta-analyses have evaluated the occurrence of lactic acidosis with the use of metformin (over 70,000 patient-years) or other antihyperglycemic agents (over 55,000 patient-years) and they have consistently shown no increase in lactic acidosis in the metformin group (35,36). In fact, CV outcomes in people with heart failure taking metformin were better than in those taking other conventional antihyperglycemic agents (37). The current evidence suggests that people with heart failure fare at least as well, if not better, with metformin than with other antihyperglycemic agents if they have only mild-to-moderate renal dysfunction (eGFR >30 mL/min) (37). As such, metformin should still be considered as first-line therapy in people with diabetes with heart failure with mild-to-moderate renal dysfunction (38).
Thiazolidinediones
Thiazolidinediones (TZDs) are known to cause fluid retention, although this is generally mild. Recent studies suggest that this is not a direct toxic effect on the myocardium. The Prospective Pioglitazone Clinical Trial In Macrovascular Events (PROACTIVE) study of pioglitazone in individuals at risk of cardiac ischemic events showed that TZDs were associated with fewer cardiac ischemic events, but at the cost of an increase in heart failure hospitalizations (2% absolute excess over 2.8 years, or <1% per year) (39). Similarly, The Diabetes Reduction Assessment With Ramipril and Rosiglitazone Medication (DREAM) study demonstrated a small excess of new-onset heart failure (0.4% absolute excess).
The RECORD trial (Rosiglitazone Evaluated for Cardiac Outcomes and Regulation of glycaemia in Diabetes) was a multicentre, open-label study that randomized 4,447 people with type 2 diabetes on metformin or sulfonylurea monotherapy to add-on rosiglitazone (n=2,220) or to a combination of metformin and sulfonylurea (n=2,227) (40). In the rosiglitazone group, the risk of heart failure death or hospitalization was doubled (HR 2.10, 95% CI 1.35–3.27): the excess heart failure event rate was 2.6 (95% CI 1.1–4.1) per 1,000 person-years. These findings confirm the increased risk of heart failure events in people treated with rosiglitazone. Since January 2012, Health Canada has advised that, “Avandia is contraindicated in patients with New York Heart Association (NYHA) Class I, II, III or IV heart failure.” Further, under serious warnings and precautions, it states that “Avandia, like other thiazolidenediones, can cause fluid retention and congestive heart failure”. A meta-analysis has not confirmed any difference in the risk of congestive heart failure (CHF) between rosiglitazone and pioglitazone (41,42).
CV outcome trials to assess for non-inferiority (CV safety) or superiority of new antihyperglycemic therapies have been undertaken in different diabetic populations with pre-specified secondary heart failure endpoints reported as mandated by the Food and Drug Administration (FDA) in December 2008. These CV safety studies include incretin agents (DPP-4 inhibitors and GLP-1 receptor agonists), as well as SGLT2 inhibitors. The mechanism of action and antihyperglycemic effects of these agents are detailed in the Pharmacologic Glycemic Management of Type 2 Diabetes in Adults chapter, p. S88. The information detailed below pertains directly to heart failure outcomes in people with diabetes. Of relevance, these trials were not heart failure trials per se and included only a small proportion of people with heart failure and reduced EF, hence the findings are limited in their generalizability to a broader heart failure population.
DPP-4 inhibitors
In the Saxagliptin Assessment of Vascular Outcomes Recorded in Patients with Diabetes Mellitus (SAVOR)–Thrombolysis in Myocardial Infarction (TIMI) 53 trial (SAVOR-TIMI 53) (43), the sitagliptin cardiovascular outcome study (TECOS) (44) and the Examination of Cardiovascular Outcomes with Alogliptin vs. Standard of Care (EXAMINE) (45), the endpoint of noninferiority, but not superiority was reached, suggesting these drugs have a neutral CV profile. There was an unexpected finding of increased hospitalization for heart failure noted with saxagliptin that was not seen in CV trials with the other DPP-4 inhibitors (46). Chronic kidney disease, elevated natriuretic peptide levels and previous heart failure were associated with an increased risk for heart failure hospitalization in SAVOR-TIMI 53. A secondary analysis of the EXAMINE trial did not demonstrate excess risk for heart failure hospitalization (46). Recent post-marketing, large registries and meta-analyses demonstrate overall neutrality for the class as a whole regarding heart failure (47). However, as a result of an excess risk demonstrated in the SAVOR-TIMI 53 trial, both the FDA and Health Canada have issued a warning for saxagliptin and heart failure, and the FDA has issued a similar warning for alogliptin. Specifically, the recommendation from the FDA for saxagliptin and alogliptin reads: “Healthcare professionals should consider discontinuing medications containing saxagliptin and alogliptin in patients who develop heart failure and monitor their diabetes control.” In Canada, the product monograph for saxagliptin states, under warnings and precautions: “Caution is warranted if ONGLYZA (saxagliptin) is used in patients with history of congestive heart failure (especially in those patients who also have renal impairment and/or history of MI)” (48).
GLP-1 receptor agonists
Three large trials investigating GLP-1 receptor agonists were recently reported. The primary outcomes are reported in the Pharmacologic Glycemic Management of Type 2 Diabetes in Adults chapter (see S88). In each trial, heart failure hospitalization was a pre-specified endpoint. The Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results (LEADER) trial (49), the Evaluation of CV outcomes in patients with type 2 diabetes after ACS using Lixisenatide (ELIXA) trial (50), and the Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes (SUSTAIN)-6 trial (51) were recently reported and demonstrated no excessive risk for heart failure hospitalization. Treatment with liraglutide in the LEADER trial was associated with a non-significant 13% reduction in heart failure hospitalization (HR 0.87, 95% CI 0.73–1.05, p=0.14), lixisenatide treatment in the ELIXA trial demonstrated a HR of 0.96, 95% CI 0.75–1.23, p=0.63) and semaglutide therapy in the SUSTAIN-6 trial demonstrated a HR of 1.11, 95% CI 0.77–1.6), with a nonsignificant p value of 0.57. Heart failure was present at baseline in ~17.8%, ~22.4% and ~23.6% of participants in LEADER, ELIXA and SUSTAIN-6, respectively. Finally, the impact of liraglutide on people with reduced EF was studied by Margulies et al. in the Functional impact of GLP-1 for Heart failure treatment (FIGHT) study. Three hundred participants (59% with diabetes) with a mean LVEF of 25% who were on evidence-based heart failure therapy were randomized to placebo or liraglutide. The primary endpoint was time to death, time to rehospitalization for heart failure and time-averaged proportional change in N-terminal pro-B-type natriuretic peptide level from baseline to 180 days. There was no difference in the primary endpoint (HR 1.10, 95% CI 0.57–2.14, p=0.78). However, in people with diabetes, the HR was 1.54 (95% CI 0.97–2.46, p=0.07) for the endpoint of death or hospitalization for heart failure. These findings suggest no benefit from liraglutide in that clinical situation (52).
SGLT2 inhibitors
The Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes (EMPA-REG OUTCOME) trial (53) demonstrated CV superiority with reduction in CV death, hospitalization for heart failure and all-cause mortality compared to placebo. While only 10.5% of participants enrolled in this study had pre-existing heart failure, there was a 35% reduction in heart failure hospitalization (p=0.0017, 95% CI 0.50–0.85). Furthermore, empagliflozin reduced the risk of heart failure hospitalization by a similar degree regardless of whether the participants had a prior history of heart failure or not. The mechanisms of benefit remains speculative. The other SGLT2 inhibitor trial with canagliflozin, CANagliflozin cardioVascular Assessment Study (CANVAS) trial (54) was recently reported. This met the prespecified noninferiority MACE endpoint and demonstrated superiority over standard care (p=0.02, HR 0.86, 95% CI 0.75–0.97). However, based on hierarchical sequential testing, the trial did not demonstrate a reduction in all-cause mortality and, therefore, all other prespecified endpoints were considered exploratory. Hospitalization for heart failure was reduced (HR 0.67, 95% CI 0.52–0.87), although not considered statistically significant. The Dapagliflozin (Multicenter Trial to Evaluate the Effect of Dapagliflozin on the Incidence of Cardiovascular Events (DECLARE-TIMI 58) will report in November 2018 (ClinicalTrials.gov Identifier: NCT01730534).
Importantly, heart failure studies will soon commence utilizing SGLT2 inhibitors irrespective of glycemia status. The effect of dapagliflozin on time to first worsening heart failure event or CV death in people with heart failure and reduced EF, irrespective of glycemic status, has begun recruiting (ClinicalTrials.gov Identifier: NCT03036124) (55) and 2 trials are underway in patients with heart failure with a preserved ejection fraction (HFpEF) and heart failure with reduced ejection fraction (HFrEF) using empagliflozin (ClinicalTrials.gov Identifier: NCT03057977 and NCT03057951) (56,57).
A detailed discussion of the rationale and evidence for the treatment approach to people with heart failure is available in the Canadian Cardiovascular Society consensus recommendations (http://www.ccsguidelineprograms.ca) (23).
Recommendations
- Individuals with diabetes and heart failure should receive the same heart failure therapies as those identified in the evidence-based Canadian Cardiovascular Society Heart Failure recommendations (http://www.onlinecjc.ca/article/S0828-282X(17)30973-X/pdf) [Grade D, Consensus (23)].
- Unless contraindicated, metformin may be used in people with type 2 diabetes and heart failure [Grade C, Level 3 (18,38)]. Metformin should be temporarily withheld if renal function acutely worsens, and should be discontinued if renal function significantly and chronically worsens [Grade D, Consensus].
- For people with NYHA class I-IV, exposure to TZDs should be avoided [Grade A, Level 1 (41)].
- Beta blockers should be prescribed when indicated for heart failure with reduced ejection fraction, as they provide similar benefits in people with or without diabetes [Grade B, Level 2 (19,33)].
- In adults with type 2 diabetes with clinical CVD in whom glycemic targets are not achieved with existing antihyperglycemic medication(s) and with an eGFR >30 mL/min/1.73 m
- In adults with diabetes and heart failure with an eGFR <60 mL/min/1.73m
- Starting doses of ACE inhibitors or ARBs should be halved [Grade D, Consensus]
- Serum electrolytes and creatinine, BP and body weight, as well as heart failure symptoms and signs, should be monitored within 7–10 days of any initiation or titration of therapy [Grade D, Consensus]
- Dose-up titration should be more gradual (with monitoring of BP, serum potassium and creatinine) [Grade D, Consensus].
Abbreviations:
A1C, glycated hemoglobin; ACE, angiotensin-converting enzyme; ACR; albumin to creatinine ratio; ARB, angiotensin receptor blocker; BNP, brain natriuretic peptide; BP, blood pressure; CI, confidence interval; CV, cardiovascular; EF, ejection fraction; eGFR; estimated glomerular filtration rate; FDA; Food and Drug Administration; HR, hazard ratio; LV, left ventricular; LVEF, left ventricular ejection fraction; NT-pro-BNP, pro-hormone of BNP; NYHA, New York Heart Association; RAAS, renin angiotensin aldosterone system; TZD, thiazolidinedione.
Other Relevant Guidelines
- Pharmacologic Glycemic Management of Type 2 Diabetes in Adults, p. S88
- Chronic Kidney Disease in Diabetes, p. S201
Literature Review Flow Diagram for Chapter 28: Treatment of Diabetes in People with Heart Failure
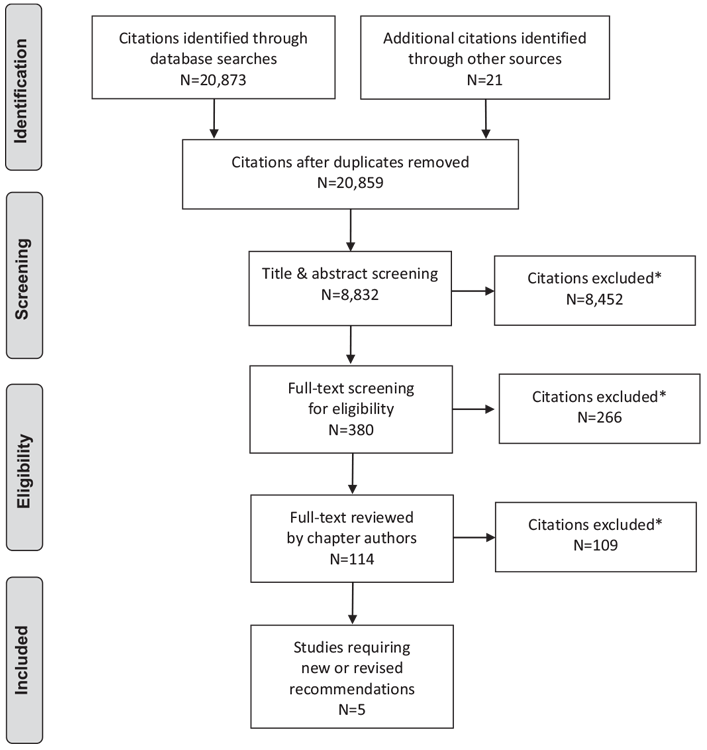
*Excluded based on: population, intervention/exposure, comparator/control or study design
From: Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6(6): e1000097. doi:10.1371/journal.pmed1000097 (58).
For more information, visit www.prisma-statement.org.
Author Disclosures
Dr. Gilbert reports grants and personal fees from AstraZeneca and Boehringer Ingelheim, and personal fees from Janssen and Merck, outside the submitted work. Dr. Liu reports grants from Servier, Roche Diagnostics, and Novo Nordisk, outside the submitted work. Dr. Connelly has nothing to disclose.
References
- Krum H, Gilbert RE. Demographics and concomitant disorders in heart failure. Lancet 2003;362:147–58.
- Albertini JP, Cohen R, Valensi P, et al. B-type natriuretic peptide, a marker of asymptomatic left ventricular dysfunction in type 2 diabetic patients. Diabetes Metab 2008;34:355–62.
- O’Donoghue M, Kenney P, Oestreicher E, et al. Usefulness of aminoterminal probrain natriuretic peptide testing for the diagnostic and prognostic evaluation of dyspneic patients with diabetes mellitus seen in the emergency department (from the PRIDE Study). Am J Cardiol 2007;100:1336–40.
- Ohkuma T, Jun M,Woodward M, et al. Cardiac stress and inflammatory markers as predictors of heart failure in patients with type 2 diabetes: The ADVANCE trial. Diabetes Care 2017;40:pii: cd170509.
- Valle R, Bagolin E, Canali C, et al. The BNP assay does not identify mild left ventricular diastolic dysfunction in asymptomatic diabetic patients. Eur J Echocardiogr 2006;7:40–4.
- Shimabukuro M, Higa N, Oshiro Y, et al. Diagnostic utility of brain-natriuretic peptide for left ventricular diastolic dysfunction in asymptomatic type 2 diabetic patients. Diabetes Obes Metab 2007;9:323–9.
- Galderisi M. Diastolic dysfunction and diabetic cardiomyopathy: Evaluation by Doppler echocardiography. J Am Coll Cardiol 2006;48:1548–51.
- Karavanaki K, Kazianis G, Konstantopoulos I, et al. Early signs of left ventricular dysfunction in adolescents with type 1 diabetes mellitus: The importance of impaired circadian modulation of blood pressure and heart rate. J Endocrinol Invest 2008;31:289–96.
- Grandi AM, Piantanida E, Franzetti I, et al. Effect of glycemic control on left ventricular diastolic function in type 1 diabetes mellitus. Am J Cardiol 2006;97:71–6.
- Ng AC, Delgado V, Bertini M, et al. Findings from left ventricular strain and strain rate imaging in asymptomatic patients with type 2 diabetes mellitus. Am J Cardiol 2009;104:1398–401.
- Mishra TK, Rath PK, Mohanty NK, et al. Left ventricular systolic and diastolic dysfunction and their relationship with microvascular complications in normotensive, asymptomatic patients with type 2 diabetes mellitus. Indian Heart J 2008;60:548–53.
- Ashraf SMS, Basir F. Association of hypertension and diastolic dysfunction with type-2 diabetes mellitus. Pakistan J Med Sci 2007;23:344–8.
- Stahrenberg R, Edelmann F, Mende M, et al. Association of glucose metabolism with diastolic function along the diabetic continuum. Diabetologi 2010;53:1331–40.
- Dinh W, Futh R, Lankisch M, et al. Cardiovascular autonomic neuropathy contributes to left ventricular diastolic dysfunction in subjects with type 2 diabetes and impaired glucose tolerance undergoing coronary angiography. Diabet Med 2011;28:311–18.
- From AM, Scott CG, Chen HH. Changes in diastolic dysfunction in diabetes mellitus over time. Am J Cardiol 2009;103:1463–6.
- Aguilar D, Deswal A, Ramasubbu K, et al. Comparison of patients with heart failure and preserved left ventricular ejection fraction among those with versus without diabetes mellitus. Am J Cardiol 2010;105:373–7.
- Ghali JK, Boehmer J, Feldman AM, et al. Influence of diabetes on cardiac resynchronization therapy with or without defibrillator in patients with advanced heart failure. J Card Fail 2007;13:769–73.
- Fantoni C, Regoli F, Ghanem A, et al. Long-term outcome in diabetic heart failure patients treated with cardiac resynchronization therapy. Eur J Heart Fail 2008;10:298–307.
- Haas SJ, Vos T, Gilbert RE, et al. Are beta-blockers as efficacious in patients with diabetes mellitus as in patients without diabetes mellitus who have chronic heart failure? A meta-analysis of large-scale clinical trials. Am Heart J 2003;146:848–53.
- McMurray JJ, Packer M, Desai AS, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med 2014;371:993–1004.
- Kristensen SL, Preiss D, Jhund PS, et al. Risk related to pre-diabetes mellitus and diabetes mellitus in heart failure with reduced ejection fraction: Insights from prospective comparison of ARNI with ACEI to determine impact on global mortality and morbidity in heart failure trial. Circ Heart Fail 2016;9:pii: e002560.
- Komajda M, Tavazzi L, Francq BG, et al. Efficacy and safety of ivabradine in patients with chronic systolic heart failure and diabetes: An analysis from the SHIFT trial. Eur J Heart Fail 2015;17:1294–301.
- Ezekowitz JA, O’Meara E, McDonald MA, et al. 2017 Comprehensive Update of the Canadian Cardiovascular Society Guidelines for the Management of Heart Failure. Can J Cardiol 2017;33:1342–433.
- Lopes RJ, Lourenco AP, Mascarenhas J, et al. Safety of spironolactone use in ambulatory heart failure patients. Clin Cardiol 2008;31:509–13.
- Desai AS, Swedberg K, McMurray JJ, et al. Incidence and predictors of hyperkalemia in patients with heart failure: An analysis of the CHARM Program. J Am Coll Cardiol 2007;50:1959–66.
- Sadjadi SA, McMillan JI, Jaipaul N, et al. A comparative study of the prevalence of hyperkalemia with the use of angiotensin-converting enzyme inhibitors versus angiotensin receptor blockers. Ther Clin Risk Manag 2009;5:547–52.
- Phillips CO, Kashani A, Ko DK, et al. Adverse effects of combination angiotensin II receptor blockers plus angiotensin-converting enzyme inhibitors for left ventricular dysfunction: A quantitative review of data from randomized clinical trials. Arch Intern Med 2007;167:1930–6.
- Raebel MA, McClure DL, Chan KA, et al. Laboratory evaluation of potassium and creatinine among ambulatory patients prescribed spironolactone: Are we monitoring for hyperkalemia? Ann Pharmacother 2007;41:193–200.
- Raebel MA, Ross C, Xu S, et al. Diabetes and drug-associated hyperkalemia: Effect of potassium monitoring. J Gen Intern Med 2010;25:326–33.
- Feuvray D, Darmellah A. Diabetes-related metabolic perturbations in cardiac myocyte. Diabetes Metab 2008;34:S3–9.
- Wenmeng W, Qizhu T. Early administration of trimetazidine may prevent or ameliorate diabetic cardiomyopathy. Med Hypotheses 2011;76:181–3.
- Belardinelli R, Cianci G, Gigli M, et al. Effects of trimetazidine on myocardial perfusion and left ventricular systolic function in type 2 diabetic patients with ischemic cardiomyopathy. J Cardiovasc Pharmacol 2008;51:611–15.
- Bell DS, Lukas MA, Holdbrook FK, et al. The effect of carvedilol on mortality risk in heart failure patients with diabetes: Results of a meta-analysis. Curr Med Res Opin 2006;22:287–96.
- Gilbert RE, Krum H. Heart failure in diabetes: Effects of anti-hyperglycaemic drug therapy. Lancet 2015;385:2107–17.
- Salpeter SR, Greyber E, Pasternak GA, et al. Risk of fatal and nonfatal lactic acidosis with metformin use in type 2 diabetes mellitus. Cochrane Database Syst Rev 2010;(4):CD002967.
- Salpeter SR, Greyber E, Pasternak GA, et al. Risk of fatal and nonfatal lactic acidosis with metformin use in type 2 diabetes mellitus: Systematic review and meta-analysis. Arch Intern Med 2003;163:2594–602.
- Andersson C, Olesen JB, Hansen PR, et al. Metformin treatment is associated with a low risk of mortality in diabetic patients with heart failure: A retrospective nationwide cohort study. Diabetologia 2010;53:2546–53.
- Eurich DT, Weir DL, Majumdar SR, et al. Comparative safety and effectiveness of metformin in patients with diabetes mellitus and heart failure: Systematic review of observational studies involving 34,000 patients. Circ Heart Fail 2013;6:395–402.
- Pfister R, Cairns R, Erdmann E, et al. A clinical risk score for heart failure in patients with type 2 diabetes and macrovascular disease: An analysis of the PROactive study. Int J Cardiol 2013;162:112–16.
- Home PD, Pocock SJ, Beck-Nielsen H, et al. Rosiglitazone evaluated for cardiovascular outcomes in oral agent combination therapy for type 2 diabetes (RECORD): A multicentre, randomised, open-label trial. Lancet 2009;373:2125–35.
- Lago RM, Singh PP, Nesto RW. Congestive heart failure and cardiovascular death in patients with prediabetes and type 2 diabetes given thiazolidinediones: A meta-analysis of randomised clinical trials. Lancet 2007;370:1129–36.
- Yacoub R, Habib H, Lahdo A, et al. Association between smoking and chronic kidney disease: A case control study. BMC Public Health 2010;10:731.
- Scirica BM, Bhatt DL, Braunwald E, et al. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N Engl J Med 2013;369:1317–26.
- Green JB, Bethel MA, Armstrong PW, et al. Effect of sitagliptin on cardiovascular outcomes in type 2 diabetes. N Engl J Med 2015;373:232–42.
- White WB, Cannon CP, Heller SR, et al. Alogliptin after acute coronary syndrome in patients with type 2 diabetes. N Engl J Med 2013;369:1327–35.
- Scirica BM, Braunwald E, Raz I, et al. Heart failure, saxagliptin, and diabetes mellitus: Observations from the SAVOR-TIMI 53 randomized trial. Circulation 2014;130:1579–88.
- Yu OH, Filion KB, Azoulay L, et al. Incretin-based drugs and the risk of congestive heart failure. Diabetes Care 2015;38:277–84.
- Product monograph Pr ONGLYZA saxagliptin tablets. Mississauga: AstraZeneca Canada Inc, 2016. https://www.astrazeneca.ca/content/dam/az-ca/downloads/ productinformation/onglyza-product-monograph-en.pdf.
- Marso SP, Daniels GH, Brown-Frandsen K, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2016;375:311–22.
- Pfeffer MA, Claggett B, Diaz R, et al. Lixisenatide in patients with type 2 diabetes and acute coronary syndrome. N Engl J Med 2015;373:2247–57.
- Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med 2016;375:1834–44.
- Margulies KB, Hernandez AF, Redfield MM, et al. Effects of liraglutide on clinical stability among patients with advanced heart failure and reduced ejection fraction: A randomized clinical trial. JAMA 2016;316:500–8.
- Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 2015;373:2117–28.
- Neal B, Perkovic V, Mahaffey KW, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med 2017;377:644–57.
- Study to evaluate the effect of dapagliflozin on the incidence of worsening heart failure or cardiovascular death in patients with chronic heart failure with reduced ejection fraction. AstraZeneca, 2017. https://clinicaltrials.gov/ct2/show/ NCT03036124.
- A phase III randomised, double-blind trial to evaluate efficacy and safety of once daily empagliflozin 10 mg compared to placebo, in patients with chronic heart failure with reduced ejection fraction (HFrEF). Boehringer Ingelheim, 2017. https://clinicaltrials.gov/ct2/show/NCT03057977.
- A phase III randomised, double-blind trial to evaluate efficacy and safety of once daily empagliflozin 10mg compared to placebo, in patients with chronic Heart Failure with preserved Ejection Fraction (HFpEF). Boehrigner Ingelheim, 2017. https://clinicaltrials.gov/ct2/show/NCT03057951.
- Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med 2009;6:e1000097.
Diabetes Canada is the registered owner of all content on guidelines.diabetes.ca and ShopDC. For questions, please email info@diabetes.ca