Chapter Headings
Key Messages for Health-care Providers
- Metabolic dysfunction–associated steatotic liver disease (MASLD) affects around 70% of people living with type 2 diabetes (T2D).
- Liver fibrosis is the primary determinant of the hepatic and nonhepatic adverse outcomes of people living with MASLD.
- Consider screening for MASLD-related liver fibrosis in all individuals living with prediabetes or type 2 diabetes by using the Fibrosis-4 Index (FIB-4) score, which can assist in ruling out the likelihood of advanced liver fibrosis.
- If the FIB-4 score is <1.3, then the management of metabolic syndrome, especially diabetes and weight, should be done in the primary care clinic. Additional tests may be required if the FIB-4 score is between 1.3 and 2.67. If the FIB-4 score is >2.67, then referral to hepatology is warranted due to the high risk of advanced fibrosis.
- Sustained weight reduction of at least 5% to 10% is recommended, but, if possible, weight loss of >10% is preferred as it can assist with reversing liver fibrosis.
- Pioglitazone and subcutaneous semaglutide may be considered to improve glycemia and may reduce the liver fat content and progression of liver fibrosis.
- Cardiovascular protection is crucial in people living with MASLD, as most people with MASLD have cardiovascular disease (CVD). Therefore, statins can be maintained unless decompensated cirrhosis is developed.
Key Messages for People Living With Diabetes
- Liver disease is common in people with diabetes. Many people living with diabetes also have a liver condition called MASLD, and many of them have not received a formal diagnosis.
- MASLD affects more than just the liver. Although it can cause liver damage over time, most people with MASLD are more likely to have heart disease, which is the leading cause of illness in this group.
- Simple blood tests can help check the liver. Everyone with prediabetes or T2D should be checked for liver scarring (also called fibrosis), which is a key predictor of complications. A simple calculation called the FIB-4 score, based on age and routine blood tests, can help rule out serious damage.
- Weight loss is one of the best treatments. Losing at least 5% to 10% of body weight can reduce fat in the liver. A 10% reduction in body weight may even help reverse some liver scarring.
- Some diabetes medications may help the liver. Certain treatments for diabetes may also reduce liver fat and slow down liver damage.
- Heart health matters too. Because heart disease is common in people with MASLD, statins (cholesterol-lowering medications) are usually safe and should be continued—except for cases of advanced liver disease like decompensated cirrhosis.
Introduction
MASLD, formerly known as nonalcoholic fatty liver disease (NAFLD), is the most common liver condition, particularly among people living with T2D. Despite its prevalence, MASLD remains underrecognized by health-care providers (HCPs) [1]. Globally, 69% of people with T2D have MASLD, and 37% have metabolic-associated steatohepatitis (MASH), highlighting the complex nature of this disease [2,3]. In contrast, MASLD affects approximately 22% of people living with type 1 diabetes mellitus (T1D) [4]. The primary drivers of MASLD are T2D and obesity [5]. Most people living with MASLD are seen in primary care or endocrinology settings, where the condition often goes undiagnosed and untreated [4]. Given its significant impact on health outcomes and the health-care system, this guideline aims to raise awareness of MASLD and provide practical recommendations for screening, diagnosis, and management in people with T2D.
Nomenclature
The terminology surrounding fatty liver disease has evolved over time. Initially termed nonalcoholic steatohepatitis (NASH) in 1980 and NAFLD in 1986 [6], this terminology was criticized for failing to fully capture the condition's underlying causes and for their potentially stigmatizing language [7]. Consequently, individuals with significant metabolic conditions, such as diabetes, obesity, and hypertension, and with fatty deposition in the liver (i.e. hepatic steatosis) who drink above the strict threshold of alcohol consumption (i.e. 30 g/day for men, 20 g/day for women), were typically excluded from this diagnosis and related clinical trials. This exclusion hindered appropriate treatment considerations [7]. In response to these concerns, the term metabolic dysfunction–associated fatty liver disease (MAFLD) was introduced. However, resistance to the inclusion of "fatty" in the nomenclature persisted. A Delphi consensus involving over 200 international experts led to a new classification system: NAFLD was renamed MASLD, whereas NASH became MASH. Both conditions (MASLD and MASH) now fall under the broader category of steatotic liver disease [7] (Figure 1). In addition, a new category called metabolic and alcohol-related liver disease (MetALD) was introduced for individuals consuming alcohol above MASLD limits but below alcoholic liver disease (ALD) thresholds (140 to 350 g/week for women, 210 to 420 g/week for men) [7]. MetALD highlights the complex interplay between metabolic dysfunction and alcohol consumption, which often coexist in real-world settings. This overlap is particularly relevant because alcohol use accelerates liver disease progression, significantly increasing the risk of liver-related events and mortality, which far exceeds the rates seen in MASLD [8]. This synergistic effect underscores the need to address both alcohol consumption and metabolic risk factors in clinical care. The recognition of MetALD also reflects the dynamic nature of liver disease, with the potential for a continuum between MASLD and ALD. Over time, either metabolic dysfunction or alcohol use may become the predominant driver of liver injury, highlighting the importance of flexible, individualized approaches to management (relevant MASLD terminologies are listed in Table 1).
Figure 1
Steatotic liver disease subclassification [7].
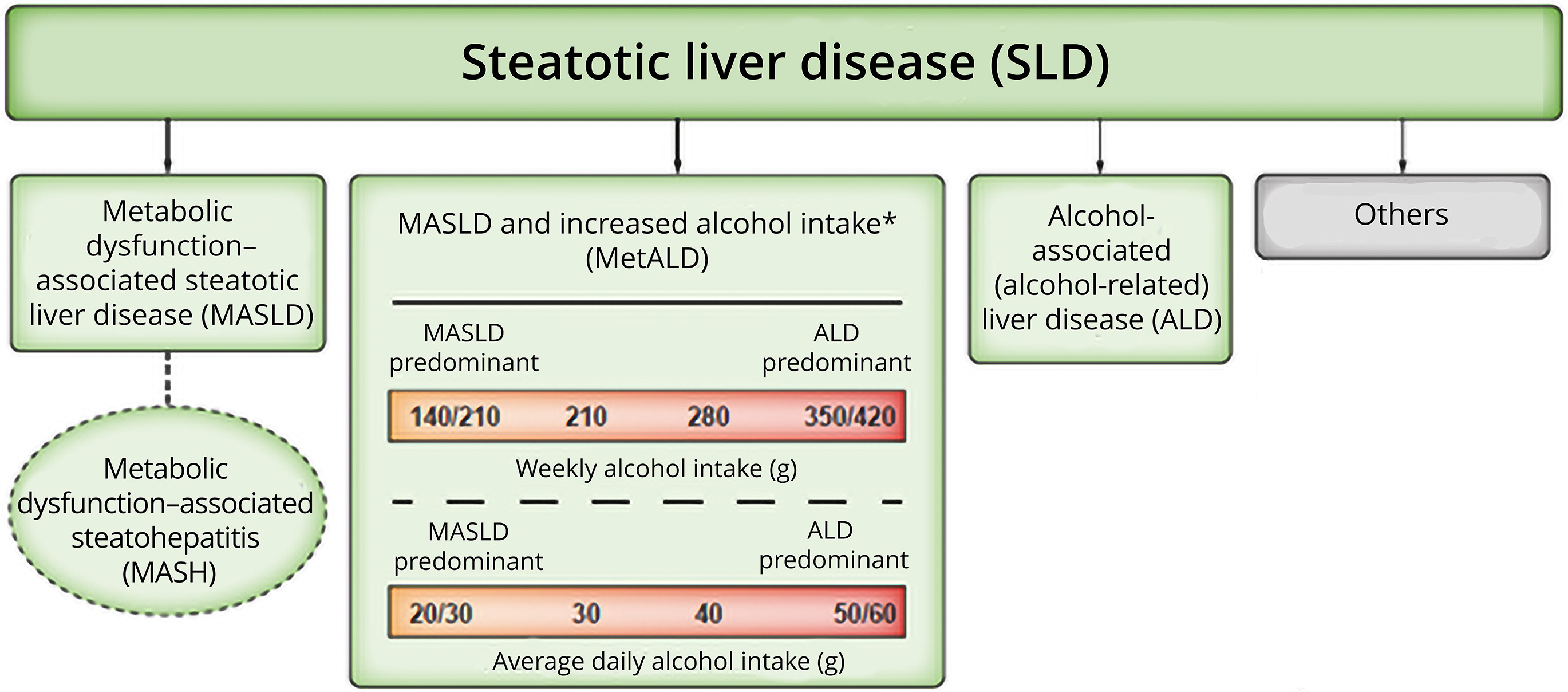
Table 1
Relevant definitions of MASLD (adapted with permission from Cusi et al [4])

Epidemiology
The global population prevalence of MASLD has risen from 25% in 2016 to 38%, with MASH now affecting 5.27% of the population [2]. In people with T2D, MASLD prevalence has increased from 55.5% to 69%, driven by rising diabetes and obesity rates worldwide [2]. Notably, 37% of individuals with T2D have MASH, with 15% developing advanced fibrosis [2,9]. A meta-analysis found that MASLD affects 22% of adults with T1D [10]. Among individuals with both obesity and diabetes, MASLD prevalence reaches 73%, but, importantly, it also affects 57% of individuals with T2D with normal body mass index (BMI) [11].
In Canada, MASLD affects 20.8% of the population, making it the most common liver disease in the country, with MASH at 5.2% [10]. Both rates are projected to increase to 22.9% and 6.5% by 2030, respectively, although these estimates are likely conservative [10]. MASLD is already the second leading cause of hepatocellular carcinoma (HCC) and liver transplants in the United States and is on track to become the primary indication for liver transplantation in Canada [11]. As MASLD prevalence rises, cases of decompensated cirrhosis, HCC, and liver transplants due to MASLD are expected to increase [10]. Increasing numbers of individuals with T2D are being evaluated for transplants related to metabolic disease–driven hepatic steatosis [12].
Although only 20% of individuals with MASH develop severe liver complications, CVD remains their leading cause of death, and many experts now consider MASLD an independent risk factor for CVD [2,13]. In addition, MASLD also increases the risk of nonhepatic gastrointestinal cancers (e.g. stomach, pancreas, esophagus, colorectal) and other malignancies (e.g. breast, lung, gynecologic) by 1.2- to 1.5-fold [13]. T2D consistently emerges as the most important risk factor for liver fibrosis, with multiple metabolic syndrome components and their duration worsening both fibrosis and clinical outcomes [11]. Therefore, a multidisciplinary care approach is recommended for managing MASLD when resources allow [14].
Methods
The Clinical Practice Guidelines (CPG) Steering Committee makes a recommendation for guideline topics at each annual cycle. A set of criteria are applied, which include scanning of internal and external guideline documents, current scientific publications, experts in the field, and emerging priorities from people living with diabetes. Additional considerations include availability of new evidence to update previous guideline chapters, the relevance of the topic to primary care providers, endocrinologists, and other HCPs involved in diabetes care, as well as overlap with other Canadian society guidelines. An annual survey of Diabetes Canada members and people living with diabetes is completed to inform this process, including suggestions from CPG Steering Committee members. The pool of potential topics is further refined based on the previously described criteria. The final curated list goes through a formal prioritization process by the CPG Steering Committee members, and the highest ranking topics are selected.
The methods process outlined in the 2018 Methods chapter of the Diabetes Canada CPG [15] was followed for the literature review, evidence appraisal, and systematic grading of recommendations. Based on their expertise, the author group was subdivided into the following subsections: introduction, including nomenclature and epidemiology; pathophysiology; diagnosis, prognosis, and screening; health behaviour interventions; use of antihyperglycemic medications; trials of MASH-targeted therapies; and vascular protection.
PICO (population, intervention, control, and outcomes) questions were developed by the authors and a systematic search of the literature was performed for relevant articles published until May 23, 2023. These can be obtained from Diabetes Canada upon request. The search was completed by health science librarians from the McMaster Evidence Review and Synthesis Team (MERST), using the MEDLINE and Embase databases. The search generated >500 unique citations. Any publications that were not found by the search but that were identified by the authors as being relevant to the topics of NAFLD, MAFLD, MASLD, and MASH were added at the title and abstract review stage. MERST reviewed all citations at the title, abstract, and full-text levels, and citations for the recommendations were critically appraised by a methodologist from MERST to assist with grading. In instances where the evidence was lacking, a Grade D Consensus grading was assigned to the recommendation.
Finally, the chapter was reviewed by a person with lived experience of T2D and MASLD to ensure it captured the perspective of individuals living with the disease. The chapter was also externally reviewed by a hepatologist and an endocrinologist, who are experts and key opinion leaders on this topic.
Pathophysiology, Risks, and Outcomes
MASLD is strongly associated with metabolic conditions, such as obesity, insulin resistance, T2D, and dyslipidemia. These conditions are interconnected through complex mechanisms, with insulin resistance playing a central role in both MASLD and T2D [16,17]. The detailed description of pathophysiology is beyond the scope of the guideline; however, the key features of MASLD pathogenesis include (Figure 2):
- Insulin resistance: Promotes hepatic steatosis by increasing free fatty acid (FFA) uptake from adipose tissue, enhancing lipogenesis and reducing triglyceride excretion [18–20].
- Progression to MASH: Oxidative stress and mitochondrial dysfunction lead to the release of inflammatory mediators, driving the transition from steatosis to metabolic-associated steatohepatitis [21,22].
- Fibrosis: Although not fully understood, lipid peroxidation activates hepatic stellate cells, resulting in fibrogenesis. This marks the final stage of MASLD progression [22].
There is a bidirectional relationship between MASLD and T2D:
- Hepatic steatosis increases the risk of developing T2D [23,24].
- T2D accelerates fibrosis progression in MASLD, worsening liver outcomes over time [23,24].
Individuals with both T2D and MASLD face higher morbidity and mortality compared to those with T2D alone:
- Increased CVD mortality is observed, even in individuals with mild fibrosis due to MASLD [25–27].
- The severity of hepatic steatosis correlates with higher risks of developing diabetes and all-cause mortality [28].
People with T2D and MASLD have significantly elevated risks of CVD, stroke, chronic kidney disease, and all-cause mortality compared to individuals with MASLD but without T2D [27,30]. They also present with heightened risks of coronary artery disease, hypertension, and diastolic dysfunction—risks that increase with advanced fibrosis stages [31,32].
CVD risk should be managed according to Diabetes Canada or American Heart Association guidelines for cardiovascular protection in people with diabetes.
Fibrosis staging (F0–F4) is critical in determining the prognosis of MASLD, as all stages, from mild (F0–F1) to significant (F2–F4) liver fibrosis, have the potential to improve with lifestyle changes. Persons with significant liver fibrosis stage (F2–F4) have an increased risk of end-stage complications. The highest risk of complications come with advanced liver fibrosis stages (F3–F4) [33] (Figure 3). Risk factors for advanced liver fibrosis include older age, male sex, Hispanic ethnicity, obesity, chronic kidney disease, and coronary artery disease [34–37]. In addition, T2D increases the risk of advanced liver fibrosis by 5- to 6-fold compared with the general population [38] and HCC by 2.5-fold, particularly after >10 years of diabetes duration [39,40]. Although noncirrhotic MASLD also raises HCC risk, routine screening is not yet recommended for these individuals [41,42].
Figure 2
Role of obesity and lipotoxicity in the development of metabolic dysfunction-associated steatohepatitis: pathophysiology and clinical implications.
ER, endoplasmic reticulum; FFA, free fatty acid; TG, triglyceride; VLDL, very-low-density lipoprotein. Adapted with permission from Cusi et al [29].
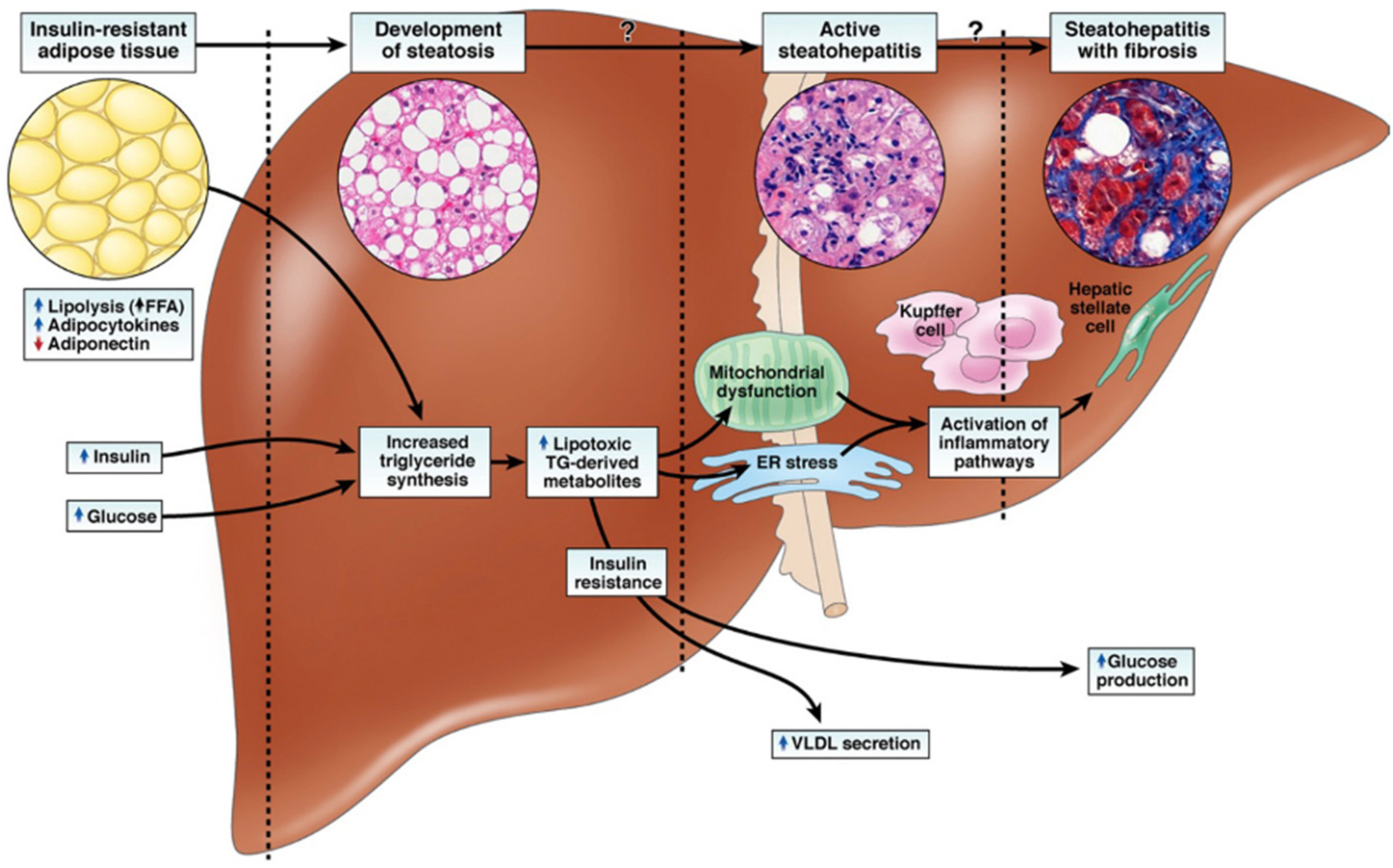
Figure 3
Spectrum of metabolic dysfunction–associated steatotic liver disease (MASLD).
MASH, metabolic-associated steatohepatitis.
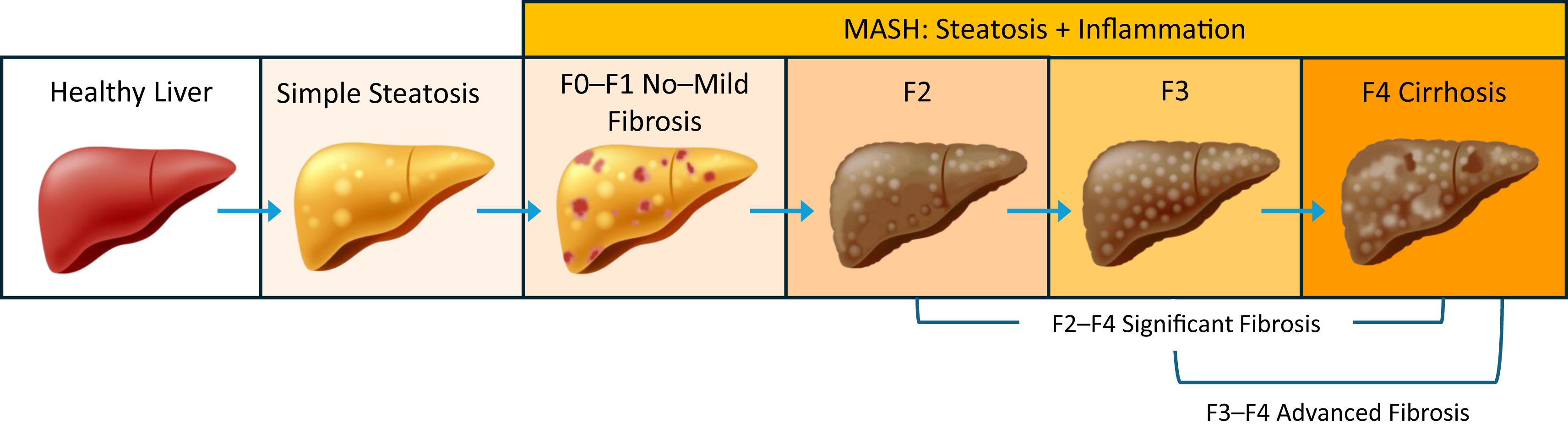
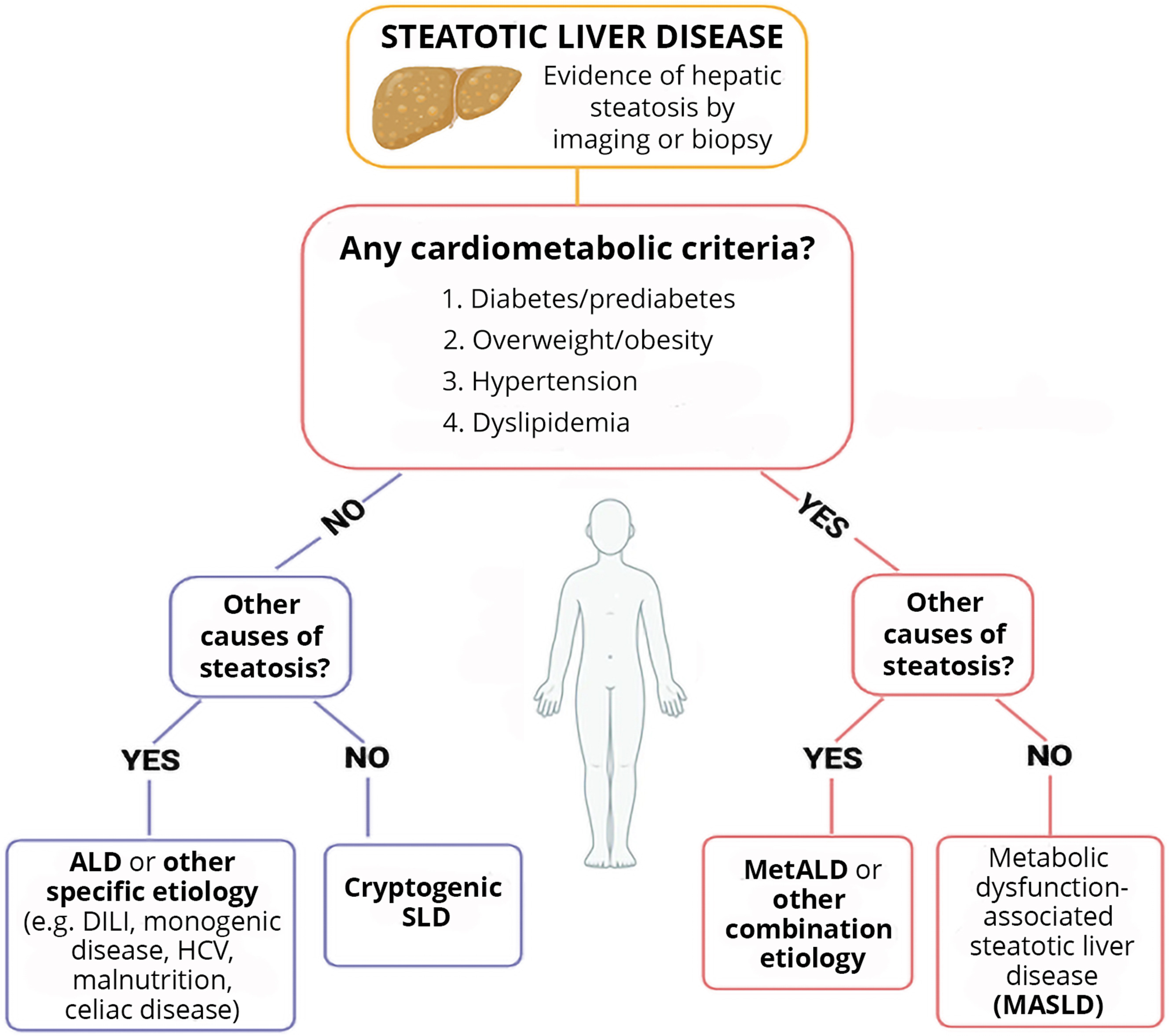
Figure 4
Algorithm for diagnosis of steatotic liver disease, including MASLD.
ALD, alcohol-associated liver disease; DILI, drug-induced liver injury; HCV, hepatitis C virus; MASLD, metabolic dysfunction–associated steatotic liver disease; MetALD, metabolic dysfunction and alcohol-related/associated steatotic liver disease; SLD, steatotic liver disease.
Diagnosis
A person with prediabetes or diabetes, with 1 additional cardiometabolic risk factor listed below, should be considered for evaluation for MASLD (Figure 4):
- Overweight or obesity: BMI >25 kg/m2 (23 kg/m2 in people of Asian ancestry) OR waist circumference >94 cm (male), 80 cm (female) OR ethnicity-adjusted equivalent.
- Hypertension: Blood pressure ≥130/80 mmHg OR on specific antihypertensive drug treatment.
- Dyslipidemia: Plasma triglyceride ≥1.70 mmol/L, plasma high-density lipoprotein (HDL) cholesterol ≤1.0 mmol/L (male), and ≤1.3 mmol/L (female) OR on lipid-lowering treatment.
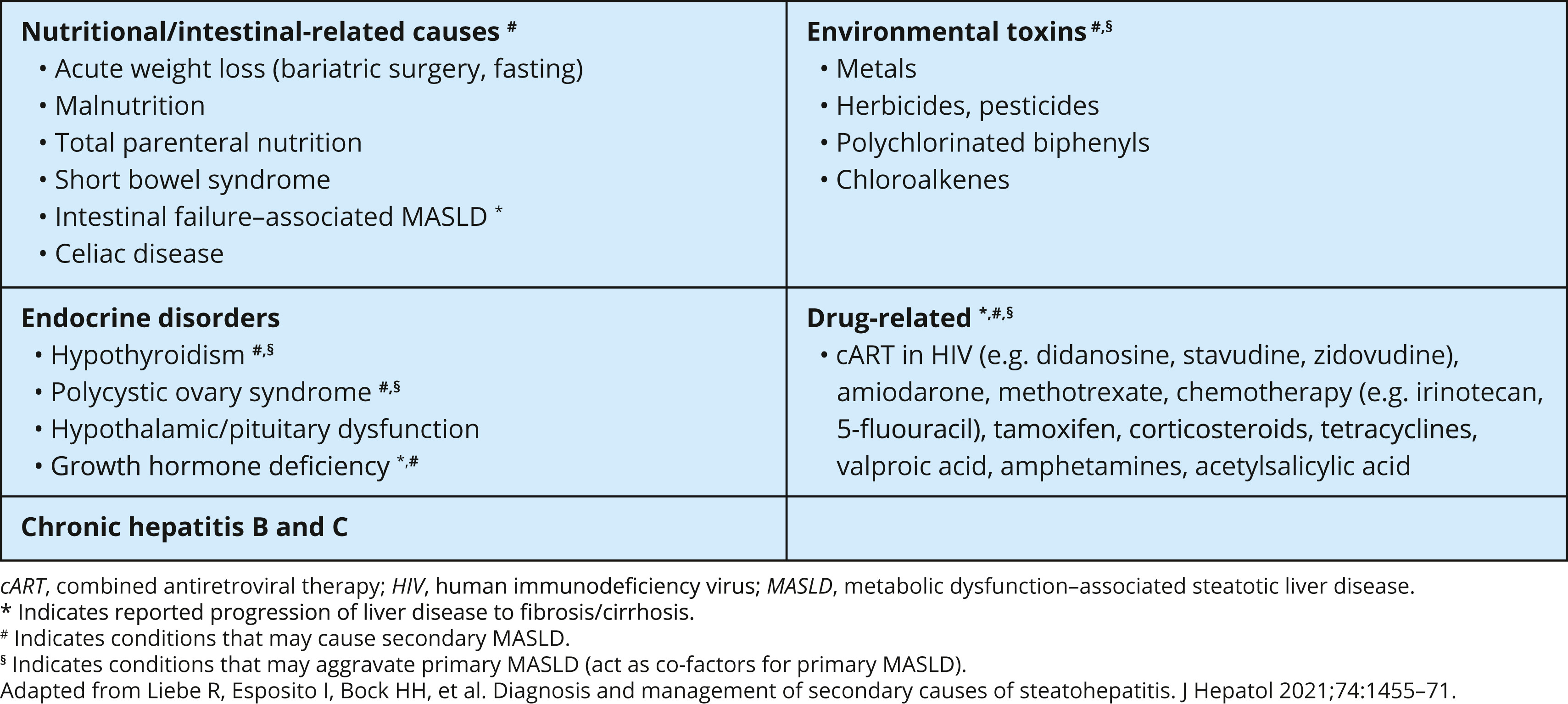
Other causes of hepatic steatosis should be considered in the absence of cardiometabolic criteria (Table 2).
Although liver biopsy remains the gold standard for diagnosing MASH and staging liver fibrosis, it is not recommended for routine use due to its invasiveness, cost, and potential sampling errors [43]. Noninvasive diagnostic tools, such as blood-based algorithms and imaging, are preferable, although clinicians should be aware that these tests may have lower performance in people with T2D [[44],[45]]. Therefore, findings from people without T2D should not be directly extrapolated to this group.
Table 2
Secondary causes of fatty liver (adapted with permission from Cusi et al) [4]
Screening
Due to the high prevalence of MASLD in T2D, screening for MASLD using radiologic investigations to detect hepatic steatosis is not recommended. Therefore, in adults with T2D, clinicians should prioritize the assessment of advanced liver fibrosis (F3–F4) due to its strong association with adverse outcomes, such as CVD, malignancy, and liver-related mortality [16,33,43,46]. Clinicians should follow evidence-based screening strategies for the early identification and management of advanced liver fibrosis in T2D to improve long-term outcomes. We recommend use of the FIB-4 score to screen for advanced liver fibrosis, as it is a simple, noninvasive, and widely available tool. A FIB-4 score is calculated using readily available clinical data, including age, platelet count, aspartate transaminase (AST) and alanine aminotransaminase (ALT) levels. Although a minority of Canadian centres may auto-calculate the FIB-4 score, clinicians can also access it through online calculators (e.g. https://www.mdcalc.com/calc/2200/fibrosis-4-fib-4-index-liver-fibrosis) (Figure 5 [47]).
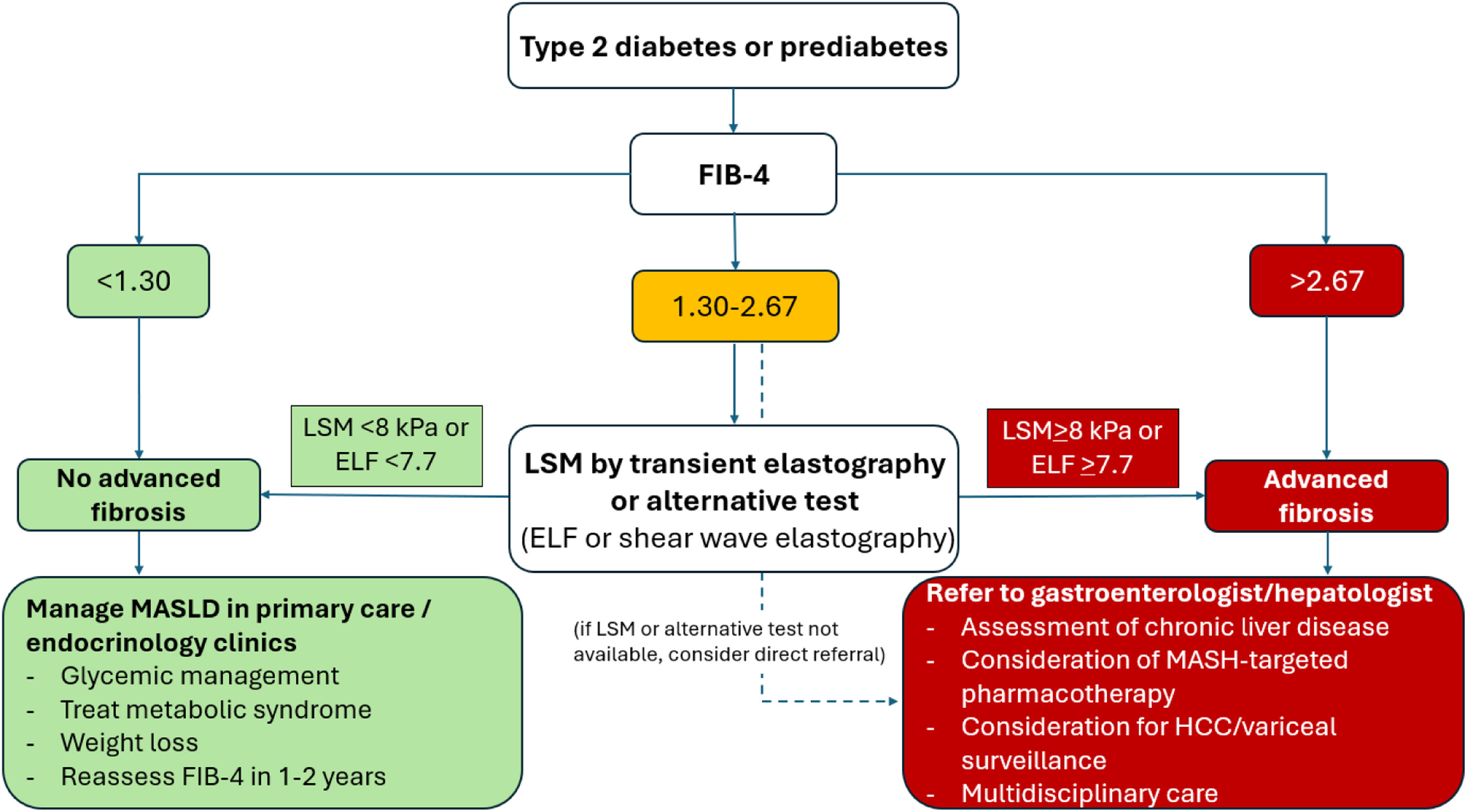
Because MASLD is often asymptomatic and transaminase levels (i.e. ALT, AST) can remain normal in up to 15% of individuals with advanced liver fibrosis, screening for advanced liver fibrosis should be performed regardless of symptoms and transaminase levels [38,48,49]. Early identification of fibrosis is essential because severity of liver fibrosis—not steatosis—is the primary driver of adverse outcomes, including cirrhosis, HCC, and liver-related mortality. Although evidence supports universal screening for advanced liver fibrosis in all individuals with T2D, those with additional risk factors, such as obesity or cardiometabolic conditions, warrant particular attention. Noninvasive care models have been developed to reduce the reliance on liver biopsy and specialist referrals [50–52]. The FIB-4 is the recommended first-line noninvasive screening tool in primary care and endocrinology settings (Figure 5). This test, which uses age, AST, ALT, and platelet count, is cost effective, easy to implement, and has high accuracy to rule out advanced liver fibrosis [53]. Its widespread adoption among individuals with prediabetes and T2D significantly reduces the need for invasive testing in low-risk populations [45,53,54]. A FIB-4 score of <1.3 suggests a low risk of advanced liver fibrosis, as it has a negative predictive value of 95% in ruling out advanced liver fibrosis when the FIB-4 score is <1.3 [53]. These individuals with low risk of fibrosis should be managed in primary care, focusing on metabolic syndrome management. For individuals with indeterminate FIB-4 scores (1.30 to 2.67), further evaluation using noninvasive liver stiffness measurement via transient elastography or enhanced liver fibrosis (ELF) biomarker testing is recommended to improve diagnostic precision [50–52]. In areas where these advanced tests are unavailable, direct referral to a gastroenterologist or hepatologist for FIB-4 scores 1.30 to 2.67 may be considered [44]. Individuals with FIB-4 scores ≥2.67, liver stiffness measurement ≥8 kPa, or ELF ≥7.7 are classified as high risk of advanced liver fibrosis and should be referred directly for specialized care due to their increased likelihood of liver-related complications [55,56] (Figure 6). Screening should be repeated every 1 to 2 years in individuals with prediabetes or T2D. Regular monitoring ensures timely detection of fibrosis progression, which can occur asymptomatically even in those with normal aminotransferase levels.
Additional blood-based algorithms, such as the NAFLD fibrosis score and AST-to-platelet ratio index have also been proposed for assessing liver fibrosis. The NAFLD fibrosis score incorporates age, BMI, diabetes status, AST, ALT, platelet count, and albumin; a score of <−1.455 effectively rules out advanced fibrosis with similar accuracy in individuals with T2D vs those without [53,54]. AST-to-platelet ratio index uses AST and platelet count but has lower accuracy than FIB-4 and the NAFLD fibrosis score in detecting advanced fibrosis in populations with T2D [57]. Despite these alternatives, FIB-4 remains the most widely used test due to its simplicity, cost-effectiveness, and validated accuracy in ruling out advanced liver fibrosis in primary care settings. Hepatic steatosis is highly prevalent among individuals with prediabetes and T2D. Its evaluation may be considered during the diagnostic and clinical assessment for advanced liver fibrosis. Although ultrasound is commonly used due to its accessibility and affordability, its sensitivity decreases in cases of mild steatosis or obesity. The controlled attenuation parameter (CAP), often paired with transient elastography, provides more accurate point-of-care assessments of steatosis, but it struggles to differentiate between grades of severity in individuals with T2D [58,59].
Magnetic resonance imaging proton density fat fraction (MRI-PDFF) offers higher precision for grading steatosis but is less accessible; thus, ultrasound and CAP remain practical options for most clinical settings [53,58]. Detecting steatosis can still help identify individuals at higher risk for MASLD progression, enabling early interventions. Managing MASLD, especially those with advanced liver fibrosis, requires a multidisciplinary approach involving hepatologists, endocrinologists, and primary care providers to address both liver health and metabolic comorbidities comprehensively. In resource-rich settings, multidisciplinary care optimizes outcomes by reducing liver-related complications. In resource-limited areas, coordinated care pathways are essential for effective disease management within local health-care capacities. In summary, systematic screening for advanced liver fibrosis in individuals with prediabetes or T2D is essential for early detection and intervention. FIB-4 serves as the cornerstone of this approach due to its simplicity and reliability, supported by secondary tests like transient elastography or ELF, when needed. Ultrasound and CAP provide additional insights into hepatic steatosis but are secondary to fibrosis assessment. Regular screening intervals coupled with a multidisciplinary care model are key to mitigating MASLD-related risks over time.
Given the rising prevalence of T2D and MASLD in Canada, standardizing screening practices for advanced liver fibrosis nationwide is imperative. Studies highlight the cost-effectiveness of using FIB-4 as a first-line test followed by transient elastography or shear wave elastography to reduce reliance on invasive procedures like liver biopsy [60,61]. Policymakers should prioritize equitable access to these noninvasive diagnostic tools across Canadian provinces to improve MASLD detection and management outcomes effectively.
In people with MASLD cirrhosis, routine surveillance to detect for the complications of cirrhosis is essential. These individuals require ultrasonography and serum alpha-fetoprotein level every 6 months to detect HCC, looking for features of clinically significant portal hypertension to identify the individuals who require upper gastrointestinal (GI) endoscopy to detect esophageal varices and clinical signs and symptoms of hepatic decompensation to optimize liver-related outcomes [62].
Figure 5
FIB-4 for liver fibrosis calculation.
ALT, alanine aminotransaminase; AST, aspartate transaminase; FIB-4, Fibrosis-4 Index. Adapted from https://www.mdcalc.com/calc/2200/fibrosis-4-fib-4-index-liver-fibrosis [47].
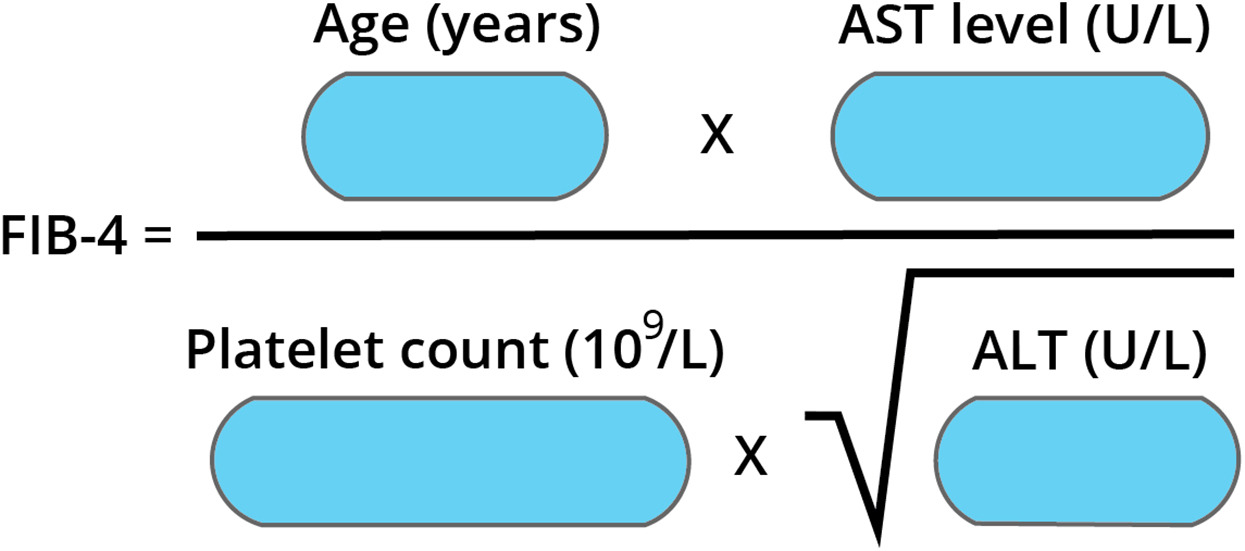
Figure 6
Overview of screening for advanced liver fibrosis and MASLD management.
ELF, enhanced liver fibrosis; FIB-4, Fibrosis-4 Index; HCC, hepatocellular carcinoma; LSM, liver stiffness measurement; MASH, metabolic-associated steatohepatitis; MASLD, metabolic dysfunction–associated steatotic liver disease.
Recommendations
- Consider screening all individuals with prediabetes or T2D, especially with the features of metabolic syndrome, for MASLD-related liver fibrosis by measuring ALT, AST, and platelets to calculate the FIB-4 score to detect advanced liver fibrosis [Grade B, Level 2] [53], rather than only measuring ALT and AST [Grade B, Level 2] [53], and identify individuals requiring further investigation, follow up, or referral (Figure 6), due to increased morbidity and mortality [Grade C, Level 3] [26–28,63].
- In individuals with low probability of advanced liver fibrosis (FIB-4 score <1.3), manage metabolic syndrome [Grade C, Level 3] [33,51,52] and consider repeat screening with FIB-4 score every 1 to 2 years [Grade D, Consensus].
- In individuals with intermediate probability of advanced liver fibrosis (FIB-4 1.30 to 2.67), additional testing, such as liver stiffness measurement (i.e. transient elastography) or alternative test (i.e. ELF), may be performed to further stratify risk [Grade B, Level 2] [53,64]. Referral to gastroenterology/hepatology may be considered if these tests are not available [Grade D, Consensus].
- In individuals with high probability of liver fibrosis (FIB-4 score ≥2.67), referral to hepatology is recommended [Grade C, Level 3] [51,65].
- In people with MASLD cirrhosis (stage F4), routine surveillance is recommended [Grade D, Level 4] [62].
- Using ultrasonography and serum alpha-fetoprotein levels every 6 months to detect HCC.
- Looking for features of clinically significant portal hypertension to identify individuals who require upper GI endoscopy to find esophageal varices.
- Clinical signs and symptoms of hepatic decompensation to optimize liver-related outcomes.
Health Behaviour Interventions
Health behaviour interventions are foundational in the prevention and management of T2D and MASLD—2 conditions often linked to poor dietary habits, sedentary lifestyle, and obesity. These interventions adopt a comprehensive approach that includes dietary modifications, physical activity, weight management, and behaviour change strategies to promote sustainable healthy habits and improve overall quality of life. An interprofessional team—comprising nurses, physicians, registered dietitians, and kinesiologists—collaborates closely with individuals living with T2D and MASLD to tailor interventions to their needs. For individuals with T2D, dietary changes, such as adopting a low-glycemic-index diet, reducing refined carbohydrates and saturated fats, and increasing fibre-rich foods, can help manage blood glucose levels and improve insulin sensitivity [66]. Regular physical activity, including aerobic exercise and resistance training, has been shown to enhance glycemic management, reduce insulin resistance, and lower cardiovascular factors [66]. Similarly, lifestyle modifications are central to MASLD management. Weight loss through calorie restriction and physical activity is the cornerstone of treatment, as it reduces liver fat accumulation, inflammation, and fibrosis [67]. Dietary patterns emphasizing whole foods—such as fruits, vegetables, lean proteins, and healthy fats—while limiting processed foods, sugary beverages (e.g. fructose-sweetened), and alcohol are recommended. Exercise further improves liver function and reduces liver fat content [67].
Obesity is a common factor in both T2D and MASLD. Weight loss not only reduces liver fat but also improves glucose regulation and insulin sensitivity [68]. Current guidelines from Canada, the United States, and Europe recommend a weight reduction of ≥5% to decrease hepatic steatosis; a 10% reduction is associated with reversing liver fibrosis [69]. For individuals with MASLD who do not have overweight or obesity, a weight loss of 3% to 5% is encouraged [68,69].
Diet and physical activity
Reducing energy intake is key to achieving weight loss; however, low-calorie diets can be challenging to sustain long-term. Calorie-unrestricted diets have emerged as alternatives for maintaining long-term weight loss. A randomized controlled trial involving individuals with T2D on a 6-month, calorie-unrestricted, low-carbohydrate, high-fat diet (20% carbohydrates, 50% to 60% fats, 25% to 30% proteins) demonstrated significant improvements in glycemic management and weight compared with those on a high-carbohydrate, low-fat diet (50% to 60% carbohydrates). However, these benefits were not sustained 3 months after the intervention [70]. Another trial showed that a carbohydrate-reduced, high-protein diet decreased hepatic fat content and improved glycemic control in participants with well-managed T2D over 6 weeks under stable body weight conditions. However, the short duration of the study limited its evaluation of long-term effects [71].
Similarly, an isocaloric dietary regimen rich in monounsaturated fatty acids combined with supervised exercise reduced hepatic fat content independent of aerobic training programs. The Look AHEAD trial demonstrated that a comprehensive 12-month lifestyle intervention—including moderate caloric restriction tailored to individual weight categories (<1,500 kcal/day for individuals weighing <114 kg, <1,800 kcal/day for those weighing >114 kg) combined with 175 minutes of moderate-intensity physical activity weekly—resulted in sustained weight loss over 10 years. This intervention reduced steatosis incidence and improved MASLD outcomes compared with standard diabetes education. Partial diabetes remission was observed in 11.5% of participants vs 2% in the control group. However, restrictive strategies carry risks, such as nutrient deficiencies or muscle mass loss, so they should be approached cautiously [72].
Bariatric surgery
Bariatric surgery has shown significant benefits for individuals with obesity-related T2D or MASLD when lifestyle modifications are not possible. Procedures, such as sleeve gastrectomy or Roux-en-Y gastric bypass, result in substantial weight loss that improves glucose regulation and reduces hepatic fat content within 1 year postsurgery. However, the short-term impact on fibrosis remains limited [73]. Although bariatric surgery offers a powerful therapeutic option for individuals with T2D and a BMI ≥35 kg/m2 who have not responded to other treatments, it requires careful patient selection due to risks, such as surgical complications or nutritional deficiencies. Bariatric surgery is not recommended for individuals with decompensated cirrhosis until long-term outcomes are better understood [73].
Nutrition supplementation
Emerging evidence highlights the potential role of supplements in managing hepatic steatosis in individuals with T2D and MASLD:
Dietary patterns
Various dietary patterns—including Mediterranean diets, low-fat diets, low-carbohydrate diets, DASH diets (Dietary Approaches to Stop Hypertension), paleo diets, and intermittent fasting—have been studied for their benefits in managing T2D and MASLD. Among these approaches:
Health behaviour interventions remain central to managing T2D and MASLD by addressing modifiable risk factors like obesity or poor dietary habits. Sustainable lifestyle changes tailored to individual needs—whether through structured exercise programs or personalized dietary plans—empower individuals to actively participate in their care while mitigating disease progression. Emerging therapies, such as nutritional supplements, hold promise but require further investigation through rigorous clinical trials before widespread adoption. Ultimately, a multidisciplinary care model that integrates evidence-based strategies will optimize outcomes for people living with these complex metabolic disorders.
Recommendations
- Individuals with T2D and MASLD-related liver fibrosis should aim for sustained reductions in body weight of 5% to 10% to improve glycemia, insulin sensitivity, and to decrease hepatic steatosis. Weight loss of ≥10% is recommended to increase the chance to reverse fibrosis [Grade B, Level 2] [72].
- Individuals with T2D and MASLD-related liver fibrosis should be supported toward healthy behaviour interventions, including physical activity and healthy dietary patterns, such as the Mediterranean diet, that best align with the individual’s values, culture, preferences, and treatment goals, allowing greatest adherence over the long term to achieve optimal glycemia and improve insulin sensitivity and components of metabolic syndrome [Grade C, Level 3] [86].
Pharmacologic Interventions
Antihyperglycemic agent use in MASH with T2D
No antihyperglycemic agent has been approved by Health Canada for the treatment of MASH. Among the antihyperglycemic agents approved for use in T2D in Canada, agents from 2 drug classes have demonstrated some improvement in MASH outcomes on paired liver biopsies, albeit in small trials: the thiazolidinedione (TZD) pioglitazone and the glucagon-like protein 1 receptor agonists (GLP-1 RAs) liraglutide and semaglutide. To date, there are no known long-term hepatic or mortality outcomes from large randomized controlled trials.
In the longest randomized controlled trial [87] with pioglitazone, 101 participants with prediabetes or T2D and biopsy-proven MASH were prescribed a hypocaloric diet (500-kcal/day deficit) and then randomly assigned to pioglitazone 45 mg/day or placebo for 18 months, followed by an 18-month, open-label phase with pioglitazone treatment. Among those randomly assigned to pioglitazone, 58% achieved the primary outcome of reduction of at least 2 points in NAFLD activity score in 2 histologic categories without worsening of fibrosis. The secondary outcome of resolution of MASH was observed in 51% of those randomized to pioglitazone treatment, which was also associated with improvement in individual histologic scores, including the fibrosis score. A meta-analysis [88] including 4 randomized, double-blind, placebo-controlled trials addressed the effects of pioglitazone in individuals with prediabetes or T2D combined with MASLD. Compared with placebo, pioglitazone significantly improved steatosis grade, inflammation grade, and degree of ballooning, whereas there was no significant improvement in liver fibrosis stage with pioglitazone compared with placebo. Low doses of pioglitazone can improve diabetes management [89] and may also be beneficial in MASH [90]. Some meta-analyses have confirmed a benefit in steatohepatitis and suggested some benefit in fibrosis [91]. Two randomized, controlled trials of GLP-1 RAs in biopsy-proven individuals with MASH have been reported. The LEAN trial [92] randomized 52 individuals with MASH to receive liraglutide 1.8 mg/day or placebo. At trial end, 45 (87%) participants had paired (baseline, 48-week) liver biopsies, received treatment, and were included in the intention-to-treat analysis of the primary outcome. Nine (39%) of 23 participants in the liraglutide group had resolution of definite MASH with no worsening of fibrosis, whereas 2 (9%) of 22 individuals on placebo had histologic improvement (relative risk 4.3, 95% confidence interval [CI] 1.04 to 17.74, p=0.019). Similar proportions of individuals with (3 of 8 [38%]) and without (6 of 15 [40%]) T2D achieved the primary outcome with liraglutide treatment, whereas both responders assigned to placebo who achieved histologic improvement did not have T2D at baseline. A randomized, placebo-controlled trial [93] with once-daily subcutaneous semaglutide over a 72-week treatment period in 320 people with biopsy-proven MASH (62% with T2D and 70% with F2 or F3 fibrosis at baseline) reported resolution of steatohepatitis in 59% of participants randomized to the higher dose (0.4 mg/day semaglutide) compared with 17% in the placebo group (p<0.001). In addition, those assigned to the higher dose GLP-1 RA had significantly reduced progression of liver fibrosis (4.9% with semaglutide 0.4 mg/day compared with 18.8% on placebo). However, semaglutide did not significantly affect the stage of liver fibrosis. An improvement in fibrosis stage occurred in 43% of the participants in the 0.4-mg group and in 33% of those in the placebo group (p=0.48).
It should be noted that the recently published phase 2 trial with tirzepatide (a dual agonist of glucose-dependent insulinotropic polypeptide and GLP-1) is not included in the current chapter recommendations because the publication date was after the literature search had already been completed. As per the conclusion of this trial, which involved participants with MASH and moderate or severe fibrosis, “treatment with tirzepatide for 52 weeks was more effective than placebo with respect to resolution of MASH without worsening of fibrosis” [94].
Sodium-glucose cotransporter-2 (SGLT2) inhibitors may improve hepatic steatosis, but do not have evidence for histologic improvement of steatohepatitis or fibrosis. The EFFECT-II study [95] investigated randomization to dapagliflozin and omega-3 carboxylic acids, individually or combined, on liver fat content in people with T2D and MASLD. In this trial, only the combination treatment reduced liver MRI-PDFF and total liver fat volume in comparison with placebo. An study from Egypt that included 240 people [96] with MASLD and T2D suggested that those randomly allocated to empagliflozin 25 mg/day had a decrease in liver fat content on MRI-PDFF compared with placebo.
In conclusion, there is some published evidence with specific antihyperglycemic agents for the treatment of MASH, but the benefits with pioglitazone and GLP-1 RAs observed to date are limited to people with MASLD without cirrhosis. Treatment advancement or adjustment for people with T2D should continue to follow the recommendations from the Diabetes Canada CPG chapter [97]. A preferential consideration for pioglitazone or subcutaneous semaglutide may be warranted in people with T2D and MASH (F2 or F3). Combination of pioglitazone and GLP-1 RA improves diabetes management and is associated with weight loss [98], and is reported to reduce hepatic steatosis and may prevent MASH progression [99]. Further information regarding non-MASLD effects, advantages, disadvantages, and precautions related to antihyperglycemic agents use in T2D is available in the Diabetes Canada guideline [97].
Recommendations
- In individuals with T2D and MASLD-related liver fibrosis (F2 or F3), pioglitazone [Grade A, Level 1A] [87,88,100] or subcutaneous semaglutide [Grade D, Level 4] [101] may be considered over other antihyperglycemic agents to achieve optimal glycemia, which may reduce steatohepatitis and progression of fibrosis.
Trials of MASH-targeted therapies
A healthy diet and regular exercise are the cornerstones of MASLD treatment in people with prediabetes or T2D [33]. Improving diet quality and increasing physical activity supports both liver health and cardiovascular health, enhancing metabolic outcomes. Some T2D medications show promise in reducing liver fat, transaminases, or fibrosis, making them valuable for glycemic management in MASLD [33].
Clinical trials for MASH have expanded rapidly, with several promising drugs currently in development. Effective therapies target hepatic steatosis, inflammation, oxidative stress, and fibrosis [102]. Strategies include insulin sensitizers, anti-inflammatory agents, antioxidants, and antifibrotic therapies, with combination approaches showing potential for enhanced outcomes [102].
Vitamin E, a liposoluble antioxidant, has demonstrated anti-inflammatory effects, achieving MASH resolution in adults and children without T2D in 2 trials, yet showing no benefit for fibrosis [103,104]. However, its use is not recommended for people with T2D due to limited efficacy and safety concerns [67,105,106]. The European Society for Clinical Nutrition and Metabolism guidelines advise its use only in individuals without diabetes with confirmed MASH.
Resmetirom, a selective thyroid hormone receptor-beta agonist, showed significant reductions in liver fat and MASH resolution in phase 2 trials [107]. In phase 3 trials (MAESTRO-NASH), resmetirom achieved MASH resolution and fibrosis improvement in people with T2D and significant fibrosis (F2–F3), leading to US Food and Drug Administration approval in March 2024 [108]. Resmetirom has not been approved by Health Canada at time of writing. Treatment monitoring for thyroid and gonadal function is recommended [109,110].
Several new agents show potential as MASH-targeted therapies. Peroxisome proliferator–activated receptor agonists, such as lanifibranor and saroglitazar, show promise for treating MASH in T2D [111–113]. Lanifibranor targets all 3 peroxisome proliferator–activated receptor isoforms, improving insulin sensitivity, and reducing hepatic steatosis, inflammation, and fibrosis. Efruxifermin, a fibroblast growth factor 21 (FGF21) analogue, and aldafermin, which targets FGF19, have shown promise in improving metabolism, reducing hepatic fat, and offering potential therapeutic benefits for MASH [114–117]. Other FGF-based therapies, such as pegozafermin, are under investigation [102,118]. Farnesoid X receptor agonists, such as tropifexor and vonafexor, modulate lipid and carbohydrate metabolism, and reduce hepatic inflammation and fibrosis. Tropifexor and vonafexor have shown promise in phase 2 studies [119–125]. Firsocostat, an acetyl-CoA carboxylase inhibitor under investigation for combination therapy, reduces liver fat content but increases plasma triglycerides [126].
The MASLD treatment landscape is rapidly evolving, with multiple agents in development targeting different disease pathways. Ongoing trials will determine the efficacy and safety of these therapies, shaping future clinical management.
Therapies for vascular protection in diabetes with MASLD
CVD is the leading cause of mortality in people living with MASLD [127]. Advanced fibrosis is associated with a higher risk of CV-related mortality, and more advanced fibrosis is more commonly found in people living with T2D and MASLD [3]. The potential pathophysiologic mechanisms linking CVD and MASLD are complex and include pathways involving insulin resistance, inflammation, increased thrombosis, microbiome alteration, etc. However, the details are beyond the scope of these guidelines [127].
- Statin: Statins have been the cornerstone of CVD prevention and management for decades. They have been widely used globally as they improve CV outcomes, especially in people with T2D who are at risk for CVD [2]. Diabetes Canada recommends the use of a statin for people with T2D to keep low-density lipoprotein at ≤2.0 mmol/L or at 50% reduction from baseline, with the alternative target being non-HDL cholesterol at ≤2.6 mmol/L or apolipoprotein B at <0.8 g/L (with tighter targets in the presence of atherosclerotic cardiovascular disease (ASCVD) as per the Canadian Cardiovascular Society lipid guidelines) for CV protection purposes [128]. We now understand the benefits of statins beyond their lipid-lowering effects, including anti-inflammatory and anticoagulation effects [129,130]. The beneficial effect of statins on MASLD is not fully understood, as statins do not seem to reduce fat content in the liver. However, it has been postulated that the risk of MASH is mitigated by lipid-lowering, antioxidant, anti-inflammatory, and antifibrotic effects [131,132]. Treatment of lipids in people with T2D should continue to follow the lipid guideline recommendations from the Canadian Cardiovascular Society (https://ccs.ca/guidelines-and-clinical-practice-update-library).
Despite the significant benefits of statins, and with multiple guidelines strongly recommending the use of statins in people with T2D due to their increased risk of CVD, statins traditionally have been underutilized. A longitudinal observational study revealed that only 55.8% of individuals with at least one indication for statin therapy were actually prescribed a statin, with even lower prescription rates observed among those living with MASLD. Thirty-seven percent of the people with MASLD and CVD were on a statin. More advanced liver disease was one of the barriers to statin prescription, which resonates with the previous research findings due to the concerns about hepatotoxicity of statins by HCPs and the people they treat [133]. However, it is essential to note that severe drug-induced liver injury from statin use is exceedingly rare [134]. Rhabdomyolysis is another side effect that causes concern [134]. Multiple studies have shown the safety of statins in compensated cirrhosis, and it is widely accepted that statins can be used safely in the compensated cirrhotic stage [134,135], although doses may need to be altered and should be discontinued or used with extreme caution in decompensated cirrhosis [7]. At the time of this guideline writing, there are no Canadian guidelines specifically guiding HCPs on discontinuing statins in the context of liver disease. After reviewing the relevant available data, the authors of this chapter recommend use of statins in people with T2D and MASLD, including compensated cirrhosis for cardiovascular risk reduction, but to discontinue use in people with decompensated cirrhosis.
- Aspirin (ASA): Platelets are the first group of cells infiltrating the liver, promoting inflammation. Preclinical studies have shown that ASA can reduce hepatic steatosis and necroinflammation while preventing fibrosis and hepatocellular carcinoma [136]. Additional effects of ASA include anti-inflammatory and antitumour effects [18]. These findings are consistent with the observational studies with ASA, which were associated with reduced risk of fibrosis progression [137] and development of HCC [138]. Most recently, a small, phase 2, double-blind, randomized controlled trial demonstrated a reduction in hepatic steatosis in cohorts using ASA 81 mg/day for 6 months [133]. More extensive studies with larger cohorts are required to identify the full effect of low-dose ASA in MASLD, especially in fibrosis progression and development of HCC. Diabetes Canada recommends use of low-dose ASA in certain populations with T2D (see the “Cardiovascular Protection in People with Diabetes” chapter) [139].
- Other potential options in the future: Both angiotensin-converting enzyme (ACE) inhibitors and angiotensin-receptor blockers (ARBs) have been associated in prevention of liver-related events, including liver cancer and cirrhosis, likely due to their anti-inflammatory, anti-immunomodulatory, and antifibrotic effects [140]. Of note, Diabetes Canada has made preferential recommendations for using ACE inhibitors and ARBs as the choice of antihypertensive agents in the presence of chronic kidney disease and/or CVD. One systematic review examining the relationship between obstructive sleep apnea (OSA) and MASLD, showed an increased prevalence of OSA in people living with MASLD, whereas severity of MASLD correlated with the severity of OSA [141]. However, the strength of evidence in these studies for guideline recommendations was weak, and larger, randomized controlled trials will be needed to firmly establish the relationship between ACE inhibitors or ARBs with MASLD, and OSA and MASLD. Therefore, we are unable to make recommendations on the use of ACE inhibitors and ARBs and actively screening and treating OSA in the context of MASLD [142].
Recommendations
- Individuals with T2D and MASLD should be treated with statins, which can be continued in the absence of decompensated liver cirrhosis, to reduce their CV risk [Grade D, Level 4] [33].
Conclusion
The high prevalence of MASLD, MASH, and advanced liver fibrosis among people with T2D highlights the critical need for comprehensive screening and management strategies. The staging of liver fibrosis is crucial as it provides essential prognostic information that guides treatment decisions and predicts individual outcomes. As such, it is recommended that all people with T2D undergo screening for advanced liver fibrosis, with the FIB-4 serving as the first-line screening tool due to its effectiveness and ease of use. The goal in primary care settings is to identify people with low risk of having advanced liver fibrosis, specifically those with an FIB-4 score of <1.30. These people can be managed by their primary care physician or endocrinologist. People found to be at risk of advanced liver fibrosis should be promptly referred to a specialist in gastroenterology or hepatology for further evaluation and management, ensuring that they receive appropriate and specialized care.
For people with liver cirrhosis resulting from MASLD, periodic surveillance for liver-related complications, such as HCC and esophageal varices, is essential to facilitate early detection and treatment. Therefore, we recommend ultrasonography and obtaining serum alpha-fetoprotein levels every 6 months to detect HCC, investigate for features of clinically significant portal hypertension via upper GI endoscopy to find the esophageal varices, and examine for the clinical signs and symptoms of hepatic decompensation to optimize liver-related outcomes.
Health behavioural interventions are the cornerstone in the management of MASLD. Promoting weight loss, adherence to a healthy eating pattern such as the Mediterranean diet, and regular physical activity can significantly improve liver health and overall metabolic control.
In addition, selection of antihyperglycemic medications with benefits for MASLD, such as pioglitazone and GLP-1 RAs, should be prioritized to enhance both glycemic management and liver outcomes. Given the increased CV risk associated with T2D and MASLD, it is imperative to conduct thorough stratification for all affected individuals. Statin therapy should be administered to all people with T2D and MASLD to manage this risk, including those with compensated cirrhosis, irrespective of liver transaminase levels. This approach ensures that CV health is adequately addressed, which is crucial for reducing morbidity and mortality in this population.
In summary, the integration of liver disease management with diabetes care is essential for improving health outcomes. By implementing comprehensive screening, appropriate referrals, surveillance of cirrhosis complications, lifestyle interventions, and targeted pharmacotherapy, HCPs can effectively address the complexities of MASLD in people with T2D, ultimately enhancing their quality of life and clinical outcomes.
Recommendations
- Consider screening all individuals with prediabetes or T2D, especially with regard to the features of metabolic syndrome for MASLD-related liver fibrosis, by measuring ALT, AST, and platelets to calculate the FIB-4 score to detect advanced liver fibrosis (Grade B, Level 2) [53], rather than only measuring ALT and AST [Grade B, Level 2] [53], and identify individuals requiring further investigation, follow up, or referral (see Figure 6) due to increased morbidity and mortality [Grade C, Level 3] [26–28,63]:
- In individuals with a low probability of advanced liver fibrosis (FIB-4 score <1.3), manage metabolic syndrome [Grade C, Level 3] [33,51,52] and consider repeat screening with FIB-4 score every 1 to 2 years [Grade D, Consensus].
- In individuals with intermediate probability of advanced liver fibrosis (FIB-4 score 1.30 to 2.67), additional testing, such as liver stiffness measurement (i.e. transient elastography) or an alternative test (i.e. ELF), may be performed to further stratify risk [Grade B, Level 2] [53,64]. Referral to gastroenterology/hepatology may be considered if these tests are not available [Grade D, Consensus].
- In individuals with a high probability of liver fibrosis (FIB-4 score ≥2.67), referral to hepatology is recommended [Grade C, Level 3] [51,65].
- In people with MASLD cirrhosis (stage F4), routine surveillance is recommended [Grade D, Level 4] by [62]:
- Using ultrasonography and serum alpha-fetoprotein levels every 6 months to detect HCC.
- Looking for features of clinically significant portal hypertension to identify individuals who require upper GI endoscopy to find esophageal varices.
- Clinical signs and symptoms of hepatic decompensation to optimize liver-related outcomes.
- Individuals with T2D and MASLD-related liver fibrosis should aim for sustained reductions in body weight of 5% to 10% to improve glycemia and insulin sensitivity and decrease hepatic steatosis. A weight loss of ≥10% is recommended to increase the chance to reverse fibrosis [Grade B, Level 2] [72].
- Individuals with T2D and MASLD-related liver fibrosis should be supported toward healthy behaviour interventions, including physical activity and healthy dietary patterns, such as the Mediterranean diet, that best align with the individual’s values, culture, preferences, and treatment goals, allowing greatest adherence over the long term to achieve optimal glycemia and improve insulin sensitivity and components of metabolic syndrome [Grade C, Level 3] [86].
- In individuals with T2D and MASLD-related liver fibrosis (F2 or F3), pioglitazone [Grade A, Level 1A] [88,89,100] or subcutaneous semaglutide [Grade D, Level 4] [101] may be considered over other antihyperglycemic agents to achieve optimal glycemia, which may reduce steatohepatitis and progression of fibrosis.
- Individuals with T2D and MASLD should be treated with statins, which can be continued in the absence of decompensated liver cirrhosis, to reduce their CV risk [Grade D, Level 4] [33].
Acknowledgments
The authors thank Jill Toffoli and Felice Cinque for their contributions to the design and development of the tables and figures.
External Reviewers
The authors also thank our external reviewers for their insightful feedback and for the lending of their time and expertise: Mark G. Swain MD, MSc, FRCPC, FAASLD, FCAHS, Kenneth Cusi MD, FACP, FACE, and David Le Clair (person with lived experience of T2D and MASLD).
Author Disclosures
G.S. has acted as a speaker for Merck, Gilead, AbbVie, Eli Lilly, and Novo Nordisk; served as an advisory board member for Merck, Novo Nordisk, GlakoSmithKline, and Gilead; and has received unrestricted research funding from Theratecnologies, Inc. J.K. has acted as a speaker for Abbott, AbbVie, AstraZeneca, Bayer, Boehringer-Ingelheim, Eisai, Eli Lilly, embecta, GSK, Janssen, Medscape, Novartis, Novo Nordisk, Pfizer, Sanofi, Searchlight Pharma, Takeda, and Teva; served as an advisory board member for Abbott, ALK, AstraZeneca, Bayer, BD, Boerhinger-Ingelheim, Eli Lilly, GSK, Janssen, Novo Nordisk, Pfizer, Sanofi, Searchlight Pharma, Takeda, Teva, and Valeo; and has received unrestricted educational grant funding from Teva. A.R. has acted as an advisor/consultant for AbbVie, Gilead, Intercept/Advanz, Janssen, Novo Nordisk, and Pfizer; received grant/research support from AbbVie, Assembly, Galmed, Gilead, Intercept/Advanz, Janssen, Merck, Novartis, Novo Nordisk, and Pfizer; and acted as a speaker for AbbVie, Amgen, Gilead, Intercept/Advanz, and Novo Nordisk. C.B. has no conflicts of interest to declare.
References
- Arrese M. Liver disease: An overlooked complication of diabetes mellitus. Nat Rev Endocrinol 2010;6:660e1.
- Younossi ZM, Golabi P, Paik JM, Henry A, Van Dongen C, Henry L. The global epidemiology of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH): A systematic review. Hepatology 2023;77:1335e47
- Younossi ZM, Golabi P, Price JK, Owrangi S, Gundu-Rao N, Satchi R, et al. The global epidemiology of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis among patients with type 2 diabetes. Clin Gastroenterol Hepatol. In press.
- Cusi K, Isaacs S, Barb D, Basu R, Caprio S, Garvey WT, et al. American Association of Clinical Endocrinology Clinical Practice Guideline for the diagnosis and management of nonalcoholic fatty liver disease in primary care and endocrinology clinical settings. Endocr Pract 2022;28:528e62.
- Kim JW, Sebastiani G. Hidden complication of obesity and diabetes—is it time to put more focus on fatty liver? Eur Med J 2023;111:77e84.
- Lonardo A, Leoni S, Alswat KA, Fouad Y. History of nonalcoholic fatty liver disease. Int J Mol Sci 2020;21:5888. https://doi.org/10.3390/ijms21165888.
- Rinella ME, Lazarus JV, Ratziu V, et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. J Hepatol 2023;6:1542e56.
- Marti-Aguado D, Calleja JL, Vilar-Gomez E, et al. Low-to-moderate alcohol consumption is associated with increased fibrosis in individuals with metabolic dysfunction-associated steatotic liver disease. J Hepatol 2024 Dec;81(6):930e940.
- Ciardullo S, Perseghin G. Prevalence of elevated liver stiffness in patients with type 1 and type 2 diabetes: A systematic review and meta-analysis. Diabetes Res Clin Pract 2022;190:109981. https://doi.org/10.1016/j.diabres.2022.109981.
- Swain MG, Ramji A, Patel K, Sebastiani G, Shaheen AA, et al. Burden of nonalcoholic fatty liver disease in Canada, 2019-2030: A modelling study. CMAJ Open 2020;8:E429e36. https://doi.org/10.9778/cmajo.20190212.
- Younossi Z, Stepanova M, Ong JP, Jacobson IM, Bugianesi E, Duseja A, et al. Nonalcoholic steatohepatitis is the fastest growing cause of hepatocellular carcinoma in liver transplant candidates. Clin Gastroenterol Hepatol 2019; 17:748e755.e3.
- Kasmi S, Artru F, Barbosa JV, Deibel AR, Favre L, Peuble C, et al. Increasing prevalence of obesity and diabetes among patients evaluated for liver transplantation in a Swiss tertiary referral center: A 10-year retrospective analysis. Swiss Med Wkly 2022 Mar 1;152:w30138. https://doi.org/10.4414/ smw.2022.w30138. PMID: 35230042.
- Mantovani A, Petracca G, Beatrice G, et al. Non-alcoholic fatty liver disease and increased risk of incident extrahepatic cancers: A meta-analysis of observational cohort studies. Gut 2022;71:778e88.
- Lazarus JV, Anstee QM, Hagström H, Cusi K, Cortez-Pinto H, Mark HE, et al. Defining comprehensive models of care for NAFLD. Nat Rev Gastroenterol Hepatol 2021;18:717e29.
- Sherifali D, Rabi D, McDonald CG, Butalia S, Campbell DJT, Hunt D, et al. Methods 2018;42(Suppl. 1):S6e9.
- Smith GI, Shankaran M, Yoshino M, et al. Insulin resistance drives hepatic de novo lipogenesis in nonalcoholic fatty liver disease. J Clinical Investigation 2020;130(3):1453e60. https://doi.org/10.1172/JCI134165.
- Bergman RN, Piccinini F, Kabir M, Kolka CM, Ader M. Hypothesis: Role of Reduced Hepatic Insulin Clearance in the Pathogenesis of Type 2 Diabetes. Diabetes 2019;68(9):1709e16. https://doi.org/10.2337/db19-0098.
- Mendez-Sanchez N, Cruz-Ramon VC, Ramirez-Perez OL, Hwang JP, BarrancoFragoso B, Cordova-Gallardo J. New aspects of lipotoxicity in nonalcoholic steatohepatitis. Int J Mol Sci. 2018 Jul 13;19(7):2034. https://doi.org/10. 3390/ijms19072034. PMID: 30011790; PMCID: PMC6073816.
- Cohen JC, Horton JD, Hobbs HH. Human fatty liver disease: Old questions and new insights. Science 2011;332:1519e23. https://doi.org/10.1126/science. 1204265.
- Pasarin M, Abraldes JG, Liguori E, Kok B, La Mura V. Intrahepatic vascular changes in non-alcoholic fatty liver disease: Potential role of insulin-resistance and endothelial dysfunction. World Journal of Gastroenterology 2017; 23(37):6777e87. https://doi.org/10.3748/wjg.v23.i37.6777.
- Day CP, James OF. Steatohepatitis: A tale of two "hits"? Gastroenterology 1998 Apr;114(4):842e5. https://doi.org/10.1016/s0016-5085(98)70599-2. PMID: 9547102.
- Enooku K, Kondo M, Fujiwara N, et al. Hepatic IRS1 and ß-catenin expression is associated with histological progression and overt diabetes emergence in NAFLD patients. Journal of Gastroenterology 2018;53(12):1261e75. https:// doi.org/10.1007/s00535-018-1472-0.
- Gastaldelli A, Cusi K. From NASH to diabetes and from diabetes to NASH: Mechanisms and treatment options. JHEP Rep 2019;1:312e28.
- Valenti L, Bugianesi E, Pajvani U, Targher G. Nonalcoholic fatty liver disease: Cause or consequence of type 2 diabetes? Liver Int 2016 Nov;36(11): 1563e79. https://doi.org/10.1111/liv.13185. Epub 2016 Jun 30. PMID: 27276701.
- Bianchi G, Marchesini G, Zoli M, Bugianesi E, Fabbri A, Pisi E. Prognostic significance of diabetes in patients with cirrhosis. Hepatology 1994;20: 119e25. https://doi.org/10.1002/hep.1840200119. PMID: 8020880.
- Stepanova M, Clement S, Wong R, Saab S, Ahmed A, Younossi ZM. Patients with diabetes and chronic liver disease are at increased risk for overall mortality: A population study from the United States. Clin Diabetes 2017;35: 79e83. https://doi.org/10.2337/cd16-0018.
- Wu W, Xiang J, Chen X. Association between diabetes mellitus and all-cause and cardiovascular mortality among individuals with ultrasound-defined non-alcoholic fatty liver disease. Front Endocrinol 2021;12:773342. https:// doi.org/10.3389/fendo.2021.773342.
- Nasr P, Fredrikson M, Ekstedt M, Kechagias S. The amount of liver fat predicts mortality and development of type 2 diabetes in non-alcoholic fatty liver disease. Liver Int 2020;40:1069e78.
- Cusi K. Role of obesity and lipotoxicity in the development of nonalcoholic steatohepatitis: Pathophysiology and clinical implications. Gastroenterology 2012;142:711e725.e6. https://doi.org/10.1053/j.gastro.2012.02.003.
- Ng CH, Chan KE, Chin YH, Zeng RW, Tsai PC, Lim WH, et al. The effect of diabetes and prediabetes on the prevalence, complications and mortality in nonalcoholic fatty liver disease. Clin Mol Hepatol 2022 Jul;28(3):565e74. https://doi.org/10.3350/cmh.2022.0096. Epub 2022 May 19. PMID: 35585687; PMCID: PMC9293620.
- Yan LH, Mu B, Guan Y, Liu X, Zhao N, Pan D, Wang SZ. Assessment of the relationship between non-alcoholic fatty liver disease and diabetic complications. J Diabetes Investig 2016 Nov;7(6):889e94. https://doi.org/10.1111/ jdi.12518. Epub 2016 Apr 20. PMID: 27181828; PMCID: PMC5089952.
- Lee M, Kim KJ, Chung TH, Bae J, Lee YH, Lee BW, et al. Nonalcoholic fatty liver disease, diastolic dysfunction, and impaired myocardial glucose uptake in patients with type 2 diabetes. Diabetes Obes Metab 2021 Apr;23(4): 1041e51. https://doi.org/10.1111/dom.14310. Epub 2021 Jan 15. PMID: 33394549.
- Rinella ME, Neuschwander-Tetri BA, Siddiqui MS, Abdelmalek MF, Caldwell S, Barb D, et al. AASLD practice guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology 2023;77: 1797e835. https://doi.org/10.1097/HEP.0000000000000323.
- Noureddin N, Noureddin M, Singh A, Alkhouri N. Progression of nonalcoholic fatty liver disease-associated fibrosis in a large cohort of patients with type 2 diabetes. Dig Dis Sci 2022 Apr;67(4):1379e88. https://doi.org/10.1007/ s10620-021-06955-x. Epub 2021 Mar 29. PMID: 33779880.
- Asero C, Giandalia A, Cacciola I, Morace C, Lorello G, Caspanello AR, et al. High prevalence of severe hepatic fibrosis in type 2 diabetic outpatients screened for non-alcoholic fatty liver disease. J Clin Med 2023 Apr 13;12(8):2858. https:// doi.org/10.3390/jcm12082858. PMID: 37109195; PMCID: PMC10146119.
- Younossi ZM, Golabi P, de Avila L, Paik JM, Srishord M, Fukui N, et al. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: A systematic review and meta-analysis. J Hepatol 2019 Oct;71(4):793e801. https://doi.org/10.1016/j.jhep.2019.06.021. Epub 2019 Jul 4. PMID: 312 79902.
- Chen J, Hu P, Wang Y, et al. Association between type 2 diabetes status and prevalence of liver steatosis and fibrosis among adults aged 40 years. BMC Endocr Discord 2022;22:128. https://doi.org/10.1186/s12902-022- 01046-y.
- Lomonaco R, Godinez Leiva E, Bril F, Shrestha S, Mansour L, Budd J, et al. Advanced liver fibrosis is common in patients with type 2 diabetes followed in the outpatient setting: The need for systematic screening. Diabetes Care 2021;44:399e406. https://doi.org/10.2337/dc20-1997.
- El-Serag HB, Hampel H, Javadi F. The association between diabetes and hepatocellular carcinoma: A systematic review of epidemiologic evidence. Clin Gastroenterol Hepatol 2006;4:369e80. https://doi.org/10.1016/j.cgh. 2005.12.007.
- Yang JD, Ahmed F, Mara KC, Addissie BD, Allen AM, Gores GJ, et al. Diabetes is associated with increased risk of hepatocellular carcinoma in patients with cirrhosis from nonalcoholic fatty liver disease. Hepatology 2020;71:907e16. https://doi.org/10.1002/hep.30858.
- Huang DQ, El-Serag HB, Loomba R. Global epidemiology of NAFLD-related HCC: Trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol 2021 Apr;18(4):223e38. https://doi.org/10.1038/s41575-020- 00381-6. Epub 2020 Dec 21. PMID: 33349658; PMCID: PMC8016738.
- Huang DQ, Noureddin N, Ajmera V, Amangurbanova M, Bettencourt R, Truong E, et al. Type 2 diabetes, hepatic decompensation, and hepatocellular carcinoma in patients with non-alcoholic fatty liver disease: An individual participant-level data meta-analysis. Lancet Gastroenterol Hepatol 2023;8:829e36. https://doi. org/10.1016/S2468-1253(23)00157-7. Erratum in: Lancet Gastroenterol Hepatol 2023;8:e7. https://doi.org/10.1016/S2468-1253(23)00234-0.
- Sterling RK, Duarte-Rojo A, Patel K, Asrani SK, Alsawas M, Dranoff JA, et al. AASLD practice guideline on imaging-based noninvasive liver disease assessment of hepatic fibrosis and steatosis. Hepatology 2025;81:672e724. https://doi.org/10.1097/HEP.0000000000000843.
- Bril F, McPhaul MJ, Caulfield MP, Clark VC, Soldevilla-Pico C, et al. Performance of plasma biomarkers and diagnostic panels for nonalcoholic steatohepatitis and advanced fibrosis in patients with type 2 diabetes. Diabetes Care 2020;43:290e7. https://doi.org/10.2337/dc19-1071.
- Boursier J, Canivet CM, Costentin C, Lannes A, Delamarre A, Sturm N, et al. Impact of type 2 diabetes on the accuracy of noninvasive tests of liver fibrosis with resulting clinical implications. Clin Gastroenterol Hepatol 2023;21: 1243e1251.e12. https://doi.org/10.1016/j.cgh.2022.02.059.
- Taylor RS, Taylor RJ, Bayliss S, Hagström H, Nasr P, Schattenberg JM, et al. Association between fibrosis stage and outcomes of patients with nonalcoholic fatty liver disease: A systematic review and meta-analysis. Gastroenterology 2020 May;158(6):1611e1625.e12. https://doi.org/10.1053/j.gastro. 2020.01.043. Epub 2020 Feb 4. PMID: 32027911.
- MDþCALC. FIB-4 index for liver fibrosis calculation. https://www.mdcalc. com/calc/2200/fibrosis-4-fib-4-index-liver-fibrosis. Accessed January 2025.
- Lomonaco R, Godinez Leiva E, Bril F, Shrestha S, Mansour L, Budd J, Portillo Romero J, et al. Advanced liver fibrosis is common in patients with type 2 diabetes followed in the outpatient setting: The need for systematic screening. Diabetes Care 2021 Feb;44(2):399e406. https://doi.org/10.2337/ dc20-1997. Epub 2020 Dec 21. PMID: 33355256; PMCID: PMC7818321.
- Harrison SA, Gawrieh S, Roberts K, Lisanti CJ, Schwope RB, Cebe KM, et al. Prospective evaluation of the prevalence of non-alcoholic fatty liver disease and steatohepatitis in a large middle-aged US cohort. J Hepatol 2021 Aug; 75(2):284e91. https://doi.org/10.1016/j.jhep.2021.02.034. Epub 2021 Mar 18. PMID: 33746083.
- Davyduke T, Tandon P, Al-Karaghouli M, Abraldes JG, Ma MM. Impact of implementing a "FIB-4 first" strategy on a pathway for patients with NAFLD referred from primary care. Hepatol Commun 2019;3:1322e33. https://doi. org/10.1002/hep4.1411.
- Srivastava A, Gailer R, Tanwar S, Trembling P, Parkes J, Rodger A, et al. Prospective evaluation of a primary care referral pathway for patients with non-alcoholic fatty liver disease. J Hepatol 2019;71:371e8. https://doi.org/ 10.1016/j.jhep.2019.03.033.
- Shaheen AA, Riazi K, Medellin A, Bhayana D, Kaplan GG, Jiang J, et al. Risk stratification of patients with nonalcoholic fatty liver disease using a case identification pathway in primary care: A cross-sectional study. CMAJ Open 2020;8:E370e6. https://doi.org/10.9778/cmajo.20200009.
- Alhinai A, Patel K, Fonseca VA, Sebastiani G. Non-invasive diagnosis of nonalcoholic fatty liver disease in patients with type 2 diabetes. J Diabetes Complications 2021;35:107978. https://doi.org/10.1016/j.jdiacomp.2021.107978.
- Bertot LC, Jeffrey GP, de Boer B, MacQuillan G, Garas G, Chin J, et al. Diabetes impacts prediction of cirrhosis and prognosis by non-invasive fibrosis models in non-alcoholic fatty liver disease. Liver Int 2018;38:1793e802. https://doi.org/10.1111/liv.13739.
- Mózes FE, Lee JA, Vali Y, Alzoubi O, Staufer K, Trauner M, et al, LITMUS investigators. Performance of non-invasive tests and histology for the prediction of clinical outcomes in patients with non-alcoholic fatty liver disease: an individual participant data meta-analysis. Lancet Gastroenterol Hepatol 2023 Aug;8(8):704e13. https://doi.org/10.1016/S2468-1253(23)00141-3. Epub 2023 Jun 5. PMID: 37290471.
- Anstee QM, Berentzen TL, Nitze LM, Jara M, Jensen AB, Kjær MS, et al. Prognostic utility of Fibrosis-4 Index for risk of subsequent liver and cardiovascular events, and all-cause mortality in individuals with obesity and/or type 2 diabetes: A longitudinal cohort study. Lancet Reg Health Eur 2023 Dec 19;36:100780. https://doi.org/10.1016/j.lanepe.2023.100780. PMID: 38188279; PMCID: PMC10769893.
- Ciardullo S, Muraca E, Perra S, Bianconi E, Zerbini F, Oltolini A, et al. Screening for non-alcoholic fatty liver disease in type 2 diabetes using noninvasive scores and association with diabetic complications. BMJ Open Diabetes Res Care 2020 Feb;8(1):e000904. https://doi.org/10.1136/bmjdrc2019-000904. PMID: 32049637; PMCID: PMC7039600.
- Petroff D, Blank V, Newsome PN, Shalimar, Voican CS, Thiele M, de Lédinghen V, et al. Assessment of hepatic steatosis by controlled attenuation parameter using the M and XL probes: An individual patient data meta-analysis. Lancet Gastroenterol Hepatol 2021 Mar;6(3):185e98. https://doi.org/10.1016/S2468-1253(20)30357-5. Epub 2021 Jan 16. PMID: 33460567.
- Cao YT, Xiang LL, Qi F, Zhang YJ, Chen Y, Zhou XQ. Accuracy of controlled attenuation parameter (CAP) and liver stiffness measurement (LSM) for assessing steatosis and fibrosis in non-alcoholic fatty liver disease: A systematic review and meta-analysis. EClinicalMedicine 2022 Jul 10;51:101547. https://doi.org/10.1016/j.eclinm.2022.101547. PMID: 35844772; PMCID: PMC9284399.
- Congly SE, Shaheen AA, Swain MG. Modelling the cost effectiveness of nonalcoholic fatty liver disease risk stratification strategies in the community setting. PLoS One 2021 May 21;16(5):e0251741. https://doi.org/10.1371/ journal.pone.0251741. PMID: 34019560; PMCID: PMC8139490.
- Park H, Yoon EL, Kim M, Kwon SH, Kim D, Cheung R, Kim HL, Jun DW. Costeffectiveness study of FIB-4 followed by transient elastography screening strategy for advanced hepatic fibrosis in a NAFLD at-risk population. Liver Int 2024 Apr;44(4):944e54. https://doi.org/10.1111/liv.15838. Epub 2024 Jan 30. PMID: 38291809.
- Singal AG, Llovet JM, Yarchoan M, Mehta N, Heimbach JK, Dawson LA, et al. AASLD Practice Guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology 2023 Dec 1;78(6):1922e65. https://doi. org/10.1097/HEP.0000000000000466. Epub 2023 May 22. Erratum in: Hepatology. 2023 Dec 1;78(6):E105. doi: 10.1097/HEP.0000000000000621. PMID: 37199193; PMCID: PMC10663390.
- Kim KS, Hong S, Han K, Park CY. Association of non-alcoholic fatty liver disease with cardiovascular disease and all cause death in patients with type 2 diabetes mellitus: Nationwide population based study. BMJ 2024;384: e076388. https://doi.org/10.1136/bmj-2023-076388.
- Arai T, Takahashi H, Seko Y, Toyoda H, Hayashi H, Yamaguchi K, et al. Accuracy of the enhanced liver fibrosis test in patients with type 2 diabetes mellitus and its clinical implications. Clin Gastroenterol Hepatol 2024;22: 789e797.e8. https://doi.org/10.1016/j.cgh.2023.11.022.
- Shaheen AA, Riazi K, Medellin A, Bhayana D, Kaplan GG, Jiang J, et al. Risk stratification of patients with nonalcoholic fatty liver disease using a case identification pathway in primary care: A cross-sectional study. CMAJ Open 2020 May 15;8(2):E370e6. https://doi.org/10.9778/cmajo.20200009. PMID: 32414883; PMCID: PMC7239637.
- Diabetes Canada Clinical Practice Guidelines Expert Committee, Sievenpiper JL, Chan CB, Dworatzek PD, Freeze C, Williams SL. Nutrition Therapy. Can J Diabetes 2018 Apr;42(Suppl 1):S64e79. https://doi.org/10. 1016/j.jcjd.2017.10.009. Erratum in: Can J Diabetes. 2019 Mar;43(2):153. doi: 10.1016/j.jcjd.2018.12.003. PMID: 29650114.
- Plauth M, Bernal W, Dasarathy S, Merli M, Plank LD, Schütz T, Bischoff SC. ESPEN guideline on clinical nutrition in liver disease. Clin Nutr 2019 Apr; 38(2):485e521. https://doi.org/10.1016/j.clnu.2018.12.022. Epub 2019 Jan 16. PMID: 30712783; PMCID: PMC6686849.
- Younossi ZM, Golabi P, de Avila L, Paik JM, Srishord M, Fukui N, et al. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: A systematic review and meta-analysis. J Hepatol 2019;71:793e801. https:// doi.org/10.1016/j.jhep.2019.06.021.
- Vilar-Gomez E, Martinez-Perez Y, Calzadilla-Bertot L, Torres-Gonzalez A, Gra-Oramas B, Gonzalez-Fabian L, Friedman SL, Diago M, Romero-Gomez M. Weight loss through lifestyle modification significantly reduces features of nonalcoholic steatohepatitis. Gastroenterology 2015 Aug;149(2):367e378. e5. https://doi.org/10.1053/j.gastro.2015.04.005. quiz e14-5. Epub 2015 Apr 10. PMID: 25865049.
- Hansen CD, Gram-Kampmann EM, Hansen JK, Hugger MB, Madsen BS, Jensen JM, et al. Effect of calorie-unrestricted low-carbohydrate, high-fat diet versus high-carbohydrate, low-fat diet on type 2 diabetes and nonalcoholic fatty liver disease: A randomized controlled trial. Ann Intern Med 2023;176: 10e21. https://doi.org/10.7326/M22-1787.
- Skytte MJ, Samkani A, Petersen AD, Thomsen MN, Astrup A, Chabanova E, et al. A carbohydrate-reduced high-protein diet improves HbA1c and liver fat content in weight stable participants with type 2 diabetes: A randomised controlled trial. Diabetologia 2019;62:2066e78. https://doi.org/10.1007/ s00125-019-4956-4.
- Lazo M, Solga SF, Horska A, Bonekamp S, Diehl AM, Brancati FL, et al. Fatty liver subgroup of the Look AHEAD research group. Effect of a 12-month intensive lifestyle intervention on hepatic steatosis in adults with type 2 diabetes. Diabetes Care 2010;33:2156e63. https://doi.org/10.2337/dc10- 0856.
- Seeberg KA, Borgeraas H, Hofso D, Smastuen MC, Kvan NP, Grimnes JO, et al. Gastric bypass versus sleeve gastrectomy in type 2 diabetes: Effects on hepatic steatosis and fibrosis a randomized controlled trial: A randomized controlled trial. Ann Intern Med 2022;175:74e83. https://doi.org/10.7326/M21-1962.
- Sangouni AA, Orang Z, Mozaffari-Khosravi H. Effect of omega-3 supplementation on cardiometabolic indices in diabetic patients with non-alcoholic fatty liver disease: A randomized controlled trial. BMC Nutr 2021;7:86. https://doi.org/10.1186/s40795-021-00490-8.
- Orang Z, Mohsenpour MA, Mozaffari-Khosravi H. Effect of omega-3 fatty acid supplementation on inflammatory markers and insulin resistance indices in patient with type 2 diabetes and nonalcoholic fatty liver: A randomized double-blind clinical trial. Obes Med 2020;19:100278. https://doi.org/10. 1016/j.obmed.2020.100278.
- Barchetta I, Del Ben M, Angelico F, Di Martino M, Fraioli A, La Torre G, et al. No effects of oral vitamin D supplementation on non-alcoholic fatty liver disease in patients with type 2 diabetes: A randomized, double-blind, placebo-controlled trial. BMC Med 2016;14:92. https://doi.org/10.1186/s12916- 016-0638-y.
- Ali Sangouni A, Abdollahi S, Mozaffari-Khosravi H. Effect of resveratrol supplementation on hepatic steatosis and cardiovascular indices in overweight subjects with type 2 diabetes: A double-blind, randomized controlled trial. BMC Cardiovasc Disord 2022;22:212. https://doi.org/10.1186/s12872- 022-02637-2.
- Zeraattalab-Motlagh S, Jayedi A, Shab-Bidar S. The effects of resveratrol supplementation in patients with type 2 diabetes, metabolic syndrome, and nonalcoholic fatty liver disease: An umbrella review of meta-analyses of randomized controlled trials. Am J Clin Nutr 2021;114:1675e85. https://doi. org/10.1093/ajcn/nqab250.
- El-Kady RR, Ali AK, El Wakeel LM, Sabri NA, Shawki MA. Nicotinamide supplementation in diabetic nonalcoholic fatty liver disease patients: Randomized controlled trial. Ther Adv Chronic Dis 2022;13:20406223221077958. https:// doi.org/10.1177/20406223221077958.
- Mansour A, Mohajeri-Tehrani MR, Samadi M, Qorbani M, Merat S, Adibi H, et al. Effects of supplementation with main coffee components including caffeine and/or chlorogenic acid on hepatic, metabolic, and inflammatory indices in patients with non-alcoholic fatty liver disease and type 2 diabetes: A randomized, double-blind, placebo-controlled, clinical trial. Nutr J 2021; 20:35. https://doi.org/10.1186/s12937-021-00694-5.
- Chen YP, Lu FB, Hu YB, Xu LM, Zheng MH, Hu ED. A systematic review and a dose-response meta-analysis of coffee dose and nonalcoholic fatty liver disease. Clin Nutr 2019 Dec;38(6):2552e7. https://doi.org/10.1016/j.clnu. 2018.11.030. Epub 2018 Dec 4. PMID: 30573353.
- Velasco N, Contreras A, Grassi B. The Mediterranean diet, hepatic steatosis and nonalcoholic fatty liver disease. Curr Opin Clin Nutr Metab Care 2014 Sep;17(5):453e7. https://doi.org/10.1097/MCO.0000000000000071. PMID: 25023188.
- Kontogianni MD, Tileli N, Margariti A, Georgoulis M, Deutsch M, Tiniakos D, Fragopoulou E, Zafiropoulou R, Manios Y, Papatheodoridis G. Adherence to the Mediterranean diet is associated with the severity of non-alcoholic fatty liver disease. Clin Nutr 2014 Aug;33(4):678e83. https://doi.org/10.1016/j. clnu.2013.08.014. Epub 2013 Sep 7. PMID: 24064253.
- Ryan MC, Itsiopoulos C, Thodis T, Ward G, Trost N, Hofferberth S, et al. The Mediterranean diet improves hepatic steatosis and insulin sensitivity in individuals with non-alcoholic fatty liver disease. J Hepatol 2013;59:138e43. https://doi.org/10.1016/j.jhep.2013.02.012.
- Evert AB, Dennison M, Gardner CD, Garvey WT, Lau KHK, MacLeod J, et al. Nutrition therapy for adults with diabetes or prediabetes: A consensus report. Diabetes Care 2019 May;42(5):731e54. https://doi.org/10.2337/ dci19-0014. Epub 2019 Apr 18. PMID: 31000505; PMCID: PMC7011201.
- Plaz Torres MC, Aghemo A, Lleo A, Bodini G, Furnari M, Marabotto E, Miele L, Giannini EG. Mediterranean Diet and NAFLD: What we know and questions that still need to be answered. Nutrients 2019 Dec 5;11(12):2971. https:// doi.org/10.3390/nu11122971. PMID: 31817398; PMCID: PMC6949938.
- Cusi K, Orsak B, Bril F, Lomonaco R, Hecht J, Ortiz-Lopez C, et al. Long-term pioglitazone treatment for patients with nonalcoholic steatohepatitis and prediabetes or type 2 diabetes mellitus: A randomized trial. Ann Intern Med 2016;165:305e15. https://doi.org/10.7326/M15-1774.
- Lian J, Fu J. Pioglitazone for NAFLD patients with prediabetes or type 2 diabetes mellitus: A meta-analysis. Front Endocrinol (Lausanne) 2021;12:615409. https://doi.org/10.3389/fendo.2021.615409. Erratum in: Front Endocrinol (Lausanne) 2022;13:840299. https://doi.org/10.3389/fendo.2022.840299.
- Aronoff S, Rosenblatt S, Braithwaite S, Egan JW, Mathisen AL, Schneider RL. Pioglitazone hydrochloride monotherapy improves glycemic control in the treatment of patients with type 2 diabetes: A 6-month randomized placebocontrolled dose-response study. The Pioglitazone 001 Study Group. Diabetes Care 2000;23:1605e11.
- Della Pepa G, Russo M, Vitale M, et al. Pioglitazone even at low dosage improves NAFLD in type 2 diabetes: Clinical and pathophysiological insights from a subgroup of the TOSCA.IT randomised trial. Diabetes Res Clin Pract 2021;178:108984.
- Musso G, Cassader M, Paschetta E, Gambino R. Thiazolidinediones and advanced liver fibrosis in nonalcoholic steatohepatitis: A meta-analysis. JAMA Intern Med 2017;177:633e40. https://doi.org/10.1001/jamainternmed.2016. 9607. Erratum in: JAMA Intern Med 2017;177:747. https://doi.org/10.1001/ jamainternmed.2017.0967.
- Armstrong MJ, Gaunt P, Aithal GP, Barton D, Hull D, Parker R, et al. Liraglutide safety and efficacy in patients with non-alcoholic steatohepatitis (LEAN): A multicentre, double-blind, randomised, placebo-controlled phase 2 study. Lancet 2016;387:679e90. https://doi.org/10.1016/S0140-6736(15)00803-X.
- Newsome PN, Buchholtz K, Cusi K, Linder M, Okanoue T, Ratziu V, et al. A placebo-controlled trial of subcutaneous semaglutide in nonalcoholic steatohepatitis. N Engl J Med 2021;384:1113e24. https://doi.org/10.1056/ nejmoa2028395.
- Gastaldelli A, Cusi K, Fernández Landó L, Bray R, Brouwers B, Rodríguez Á. Effect of tirzepatide versus insulin degludec on liver fat content and abdominal adipose tissue in people with type 2 diabetes (SURPASS-3 MRI): A substudy of the randomised, open-label, parallel-group, phase 3 SURPASS-3 trial. Lancet Diabetes Endocrinol 2022;10:393e406.
- Eriksson JW, Lundkvist P, Jansson PA, et al. Effects of dapagliflozin and n-3 carboxylic acids on non-alcoholic fatty liver disease in people with type 2 diabetes: A double-blind randomised placebo-controlled study. Diabetologia 2018;61:1923e34.
- Elhini SH, Wahsh EA, Elberry AA, El Ameen NF, Abdelfadil Saedii A, Refaie SM, et al. The impact of an SGLT2 inhibitor versus ursodeoxycholic acid on liver steatosis in diabetic patients. Pharmaceuticals 2022;15:1516. https://doi.org/10.3390/ph15121516.
- Shah BR, Bajaj HS, Leung K, Mansell K, Simpson S, et al. Pharmacologic glycemic management of type 2 diabetes in adults: 2024 update. Can J Diabetes 2024;48:415e24.
- Ahrén B, Masmiquel L, Kumar H, et al. Efficacy and safety of once-weekly semaglutide versus once-daily sitagliptin as an add-on to metformin, thiazolidinediones, or both, in patients with type 2 diabetes (SUSTAIN 2): A 56- week, double-blind, phase 3a, randomised trial. Lancet Diabetes Endocrinol 2017;5:341e54.
- Sathyanarayana P, Jogi M, Muthupillai R, Krishnamurthy R, Samson SL, Bajaj M. Effects of combined exenatide and pioglitazone therapy on hepatic fat content in type 2 diabetes. Obesity (Silver Spring) 2011;19:2310e5.
- Musso G, Cassader M, Paschetta E, Gambino R. Thiazolidinediones and advanced liver fibrosis in nonalcoholic steatohepatitis: A meta-analysis. JAMA Intern Med 2017 May 1;177(5):633e40. https://doi.org/10.1001/ jamainternmed.2016.9607. Erratum in: JAMA Intern Med. 2017 May 1; 177(5):747. doi: 10.1001/jamainternmed.2017.0967. PMID: 28241279; PMCID: PMC5470366.
- Newsome PN, Buchholtz K, Cusi K, Linder M, Okanoue T, Ratziu V, Sanyal AJ, Sejling AS, Harrison SA, NN9931-4296 Investigators. A placebo-controlled trial of subcutaneous semaglutide in nonalcoholic steatohepatitis. N Engl J Med 2021 Mar 25;384(12):1113e24. https://doi.org/10.1056/NEJMoa2028395. Epub 2020 Nov 13. PMID: 33185364.
- Dufour JF, Anstee QM, Bugianesi E, Harrison S, Loomba R, Paradis V, Tilg H, Wong VW, Zelber-Sagi S. Current therapies and new developments in NASH. Gut 2022 Jun 16;71(10):2123e34. https://doi.org/10.1136/gutjnl-2021- 326874. Epub ahead of print. PMID: 35710299; PMCID: PMC9484366.
- Sanyal AJ, Chalasani N, Kowdley KV, McCullough A, Diehl AM, Bass NM, et al, NASH CRN. Pioglitazone, vitamin E, or placebo for nonalcoholic steatohepatitis. N Engl J Med 2010 May 6;362(18):1675e85. https://doi.org/10.1056/NEJMoa0907929. Epub 2010 Apr 28. PMID: 20427778; PMCID: PMC2928471.
- Lavine JE, Schwimmer JB, Van Natta ML, Molleston JP, Murray KF, Rosenthal P, et al. Nonalcoholic Steatohepatitis Clinical Research Network. Effect of vitamin E or metformin for treatment of nonalcoholic fatty liver disease in children and adolescents: The TONIC randomized controlled trial. JAMA 2011 Apr 27;305(16):1659e68. https://doi.org/10.1001/jama.2011. 520. PMID: 21521847; PMCID: PMC3110082.
- Lavine JE, Schwimmer JB, Van Natta ML, Molleston JP, Murray KF, Rosenthal P, et al. Nonalcoholic Steatohepatitis Clinical Research Network. Effect of vitamin E or metformin for treatment of nonalcoholic fatty liver disease in children and adolescents: The TONIC randomized controlled trial. JAMA 2011 Apr 27;305(16):1659e68. https://doi.org/10.1001/jama.2011. 520. PMID: 21521847; PMCID: PMC3110082.
- Mazhar IJ, Yasir M, Sarfraz S, Shlaghya G, Narayana SH, Mushtaq U, et al. Vitamin E and pioglitazone: A comprehensive systematic review of their efficacy in nonalcoholic fatty liver disease. Cureus 2023 Aug 17;15(8):e43635. https://doi.org/ 10.7759/cureus.43635. PMID: 37719477; PMCID: PMC10504864.
- Harrison SA, Bashir MR, Guy CD, Zhou R, Moylan CA, Frias JP, et al. Resmetirom (MGL-3196) for the treatment of non-alcoholic steatohepatitis: A multicentre, randomised, double-blind, placebo-controlled, phase 2 trial. Lancet 2019;394: 2012e24. https://doi.org/10.1016/S0140-6736(19)32517-6.
- Cusi K, Isaacs S, Barb D, Basu R, Caprio S, Garvey WT, Kashyap S, et al. American Association of Clinical Endocrinology Clinical Practice Guideline for the Diagnosis and Management of Nonalcoholic Fatty Liver Disease in Primary Care and Endocrinology Clinical Settings: Co-Sponsored by the American Association for the Study of Liver Diseases (AASLD). Endocr Pract 2022 May;28(5):528e62. https://doi.org/10.1016/j.eprac.2022.03.010. PMID: 35569886.
- Chen VL, Morgan TR, Rotman Y, Patton HM, Cusi K, Kanwal F, et al. Resmetirom therapy for metabolic dysfunction-associated steatotic liver disease: October 2024 updates to AASLD Practice Guidance. Hepatology 2025;81:312e20.
- Cusi K. Selective agonists of thyroid hormone receptor beta for the treatment of NASH. N Engl J Med 2024;390:559e61. https://doi.org/10.1056/nejme2314365.
- Francque SM, Bedossa P, Ratziu V, Anstee QM, Bugianesi E, Sanyal AJ, et al. A randomized, controlled trial of the pan-PPAR agonist lanifibranor in NASH. N Engl J Med 2021;385:1547e58. https://doi.org/10.1056/nejmoa2036205.
- Raggi P, Milic J, Manicardi M, Cinque F, Swain MG, Sebastiani G, Guaraldi G. Metabolic dysfunction-associated steatotic liver disease: An opportunity for collaboration between cardiology and hepatology. Atherosclerosis 2024 May;392:117523. https://doi.org/10.1016/j.atherosclerosis.2024.117523. Epub 2024 Mar 16. PMID: 38522165.
- Gawrieh S, Noureddin M, Loo N, Mohseni R, Awasty V, Cusi K, Kowdley KV, Lai M, Schiff E, Parmar D, Patel P, Chalasani N. Saroglitazar, a PPAR-a/g Agonist, for Treatment of NAFLD: A Randomized Controlled Double-Blind Phase 2 Trial. Hepatology 2021 Oct;74(4):1809e24. https://doi.org/10.1002/ hep.31843. Epub 2021 Jul 19. PMID: 33811367.
- Harrison SA, Ruane PJ, Freilich BL, Neff G, Patil R, Behling CA, et al. Efruxifermin in non-alcoholic steatohepatitis: A randomized, double-blind, placebo-controlled, phase 2a trial. Nat Med 2021;27:1262e71. https://doi.org/ 10.1038/s41591-021-01425-3.
- Harrison SA, Ruane PJ, Freilich BL, Neff G, Patil R, Behling CA, et al. Efruxifermin in non-alcoholic steatohepatitis: A randomized, double-blind, placebo-controlled, phase 2a trial. Nat Med 2021;27:1262e71. https://doi.org/ 10.1038/s41591-021-01425-3.
- Harrison SA, Neff G, Guy CD, Bashir MR, Paredes AH, Frias JP, et al. Efficacy and safety of aldafermin, an engineered FGF19 analog, in a randomized, double-blind, placebo-controlled trial of patients with nonalcoholic steatohepatitis. Gastroenterology 2021;160:219e231.e1. https://doi.org/10.1053/j. gastro.2020.08.004.
- Harrison SA, Abdelmalek MF, Neff G, Gunn N, Guy CD, Alkhouri N, et al. Aldafermin in patients with non-alcoholic steatohepatitis (ALPINE 2/3): A randomised, double-blind, placebo-controlled, phase 2b trial. Lancet Gastroenterol Hepatol 2022;7:603e16. https://doi.org/10.1016/S2468-1253(22)00017-6.
- Loomba R, Lawitz EJ, Frias JP, Ortiz-Lasanta G, Johansson L, Franey BB, et al. Safety, pharmacokinetics, and pharmacodynamics of pegozafermin in patients with non-alcoholic steatohepatitis: A randomised, double-blind, placebo-controlled, phase 1b/2a multiple-ascending-dose study. Lancet Gastroenterol Hepatol 2023;8:120e32. https://doi.org/10.1016/S2468- 1253(22)00347-8.
- Lefebvre P, Cariou B, Lien F, Kuipers F, Staels B. Role of bile acids and bile acid receptors in metabolic regulation. Physiol Rev 2009 Jan;89(1):147e91. https://doi.org/10.1152/physrev.00010.2008. PMID: 19126757.
- Arab JP, Karpen SJ, Dawson PA, Arrese M, Trauner M. Bile acids and nonalcoholic fatty liver disease: Molecular insights and therapeutic perspectives. Hepatology 2017 Jan;65(1):350e62. https://doi.org/10.1002/hep.28709. Epub 2016 Aug 4. PMID: 27358174; PMCID: PMC5191969.
- Rinella ME, Dufour JF, Anstee QM, Goodman Z, Younossi Z, Harrison SA, et al. Non-invasive evaluation of response to obeticholic acid in patients with NASH: Results from the REGENERATE study. J Hepatol 2022 Mar;76(3):536e48. https:// doi.org/10.1016/j.jhep.2021.10.029. Epub 2021 Nov 15. PMID: 34793868.
- Sanyal AJ, Ratziu V, Loomba R, Anstee QM, Kowdley KV, Rinella ME, Sheikh MY, et al. Results from a new efficacy and safety analysis of the REGENERATE trial of obeticholic acid for treatment of pre-cirrhotic fibrosis due to non-alcoholic steatohepatitis. J Hep 2023;79(5):1110e20.
- Sanyal AJ, Lopez P, Lawitz EJ, Lucas KJ, Loeffler J, Kim W, et al. Tropifexor for nonalcoholic steatohepatitis: an adaptive, randomized, placebo-controlled phase 2a/b trial. Nat Med 2023 Feb;29(2):392e400. https://doi.org/10.1038/ s41591-022-02200-8. Epub 2023 Feb 16. PMID: 36797481; PMCID: PMC9941046.
- Ratziu V, Harrison SA, Loustaud-Ratti V, Bureau C, Lawitz E, Abdelmalek M, et al. Hepatic and renal improvements with FXR agonist vonafexor in individuals with suspected fibrotic NASH. J Hepatol 2023 Mar;78(3):479e92. https://doi.org/10.1016/j.jhep.2022.10.023. Epub 2022 Nov 9. PMID: 36334688.
- Alkhouri N, Herring R, Kabler H, Kayali Z, Hassanein T, Kohli A, et al. Safety and efficacy of combination therapy with semaglutide, cilofexor and firsocostat in patients with non-alcoholic steatohepatitis: A randomised, openlabel phase II trial. J Hepatol 2022 Sep;77(3):607e18. https://doi.org/10. 1016/j.jhep.2022.04.003. Epub 2022 Apr 16. PMID: 35439567.
- Loomba R, Kayali Z, Noureddin M, Ruane P, Lawitz EJ, Bennett M, et al. GS0976 Reduces Hepatic Steatosis and Fibrosis Markers in Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2018 Nov;155(5): 1463e1473.e6. https://doi.org/10.1053/j.gastro.2018.07.027. Epub 2018 Jul 27. PMID: 30059671; PMCID: PMC6318218.
- Caussy C, Aubin A, Loomba R. The relationship between type 2 diabetes, NAFLD, and cardiovascular risk. Curr Diab Rep 2021 Mar 19;21(5):15. https://doi.org/10. 1007/s11892-021-01383-7. PMID: 33742318; PMCID: PMC8805985.
- Mancini GB, Hegele RA, Leiter LA. Diabetes Canada 2018 clinical practice guidelines for the prevention and management of diabetes in Canada: Dyslipidemia. Can J Diabetes 2018;42(Suppl. 1):S178e85.
- Diamantis E, Kyriakos G, Quiles-Sanchez LV, Farmaki P, Troupis T. The antiinflammatory effects of statins on coronary artery disease: An updated review of the literature. Curr Cardiol Rev 2017;13:209e16. https://doi.org/ 10.2174/1573403X13666170426104611.
- Siniscalchi C, Basaglia M, Riva M, Meschi M, Meschi T, Castaldo G, et al. Statins effects on blood clotting: A review. Cells 2023;12:2719. https://doi. org/10.3390/cells12232719.
- Ayada I, van Kleef LA, Zhang H, Liu K, Li P, Abozaid YJ, et al. Dissecting the multifaceted impact of statin use on fatty liver disease: A multidimensional study. EBioMedicine 2023;87:104392.
- Dongiovanni P, Petta S, Mannisto V, et al. Statin use and non-alcoholic steatohepatitis in at risk individuals. J Hepatol 2015;63:705e12.
- Simon TG, Wilechansky RM, et al. Aspirin for metabolic dysfunction associated steatotic liver disease without cirrhosis. JAMA 2024;331:920e9.
- Thomson MJ, Serper M, Khungar V, et al. Prevalence and factors associated with statin use among patients with nonalcoholic fatty liver disease in the TARGET-NASH Study. Clin Gastroenterol Hepatol 2022;20: 458e460.e4.
- Gratacós-Ginès J, Pose E. Review of the role of statins in cirrhosis and portal hypertension. Clin Liver Dis 2023;22:50e7. https://doi.org/10.1097/CLD. 0000000000000015.
- Francis P, Forman L. Use of Statins in Patients With and Without Liver Disease. Clin Liver Dis (Hoboken) 2020 Feb 25;15(1):40e5.
- Simon TG, Henson J, Osganian S, et al. Daily aspirin use associated with reduced risk for fibrosis progression in patients with nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol 2019;17:2776e2784.e4. https://doi.org/ 10.1016/j.cgh.2019.04.061.
- Memel ZN, Arvind A, Moninuola O, Philpotts L, Chung RT, Corey KE, et al. Aspirin use is associated with a reduced incidence of hepatocellular carcinoma: A systematic review and meta-analysis. Hepatol Commun 2020;5: 133e43. https://doi.org/10.1002/hep4.1640.
- Stone JA, Houlden RL, Lin P, Udell JA, Verma S. Diabetes Canada 2018 Clinical Practice Guidelines for the prevention and management of diabetes in Canada: Cardiovascular protection in people with diabetes. Can J Diabetes 2018;42(Suppl.):S162e9.
- Noureddin M, Abdelmalek M. ACE inhibitors: The secret to prevent cirrhosis complications and HCC in NAFLD? Hepatology 2022;76:295e7. https://doi. org/10.1002/hep.32399.
- Umbro I, Fabiani V, Fabiani M, Angelico F, Del Ben M. Association between non-alcoholic fatty liver disease and obstructive sleep apnea. World J Gastroenterol 2020;26:2669e81. https://doi.org/10.3748/wjg. v26.i20.2669.
- Lipscombe L, Butalia S, Dasgupta K, et al. Diabetes Canada 2018 Clinical Practice Guidelines for the prevention and management of diabetes in Canada: Pharmacologic glycemic management of type 2 diabetes in adults: 2020 update. Can J Diabetes 2022;44:575e91.
Diabetes Canada is the registered owner of all content on guidelines.diabetes.ca and ShopDC. For questions, please email info@diabetes.ca