Chapter Headings
- Introduction
- Discussing DIY AID as a Therapeutic Option
- Preparing PWD for a Successful Transition to DIY AID
- Navigating DIY AID to Optimize Settings
- Future Developments
- Frequently Asked Questions
- Supplementary Material
- Author Disclosures
- Appendix A: Tidepool Key Report Guide (for Loop)
- Appendix B: Nightscout Key Report Guide
Introduction
The key message of the Diabetes Canada position statement on do-it-yourself automated insulin delivery (DIY AID) is that clinicians should support people living with type 1 diabetes (T1D) and their caregivers in whichever method of insulin delivery they choose (for the purpose of this guide, PWD will refer to people with T1D and their caregivers). This health-care practitioner (HCP) user's guide is being published alongside the position statement to provide clinicians with guidance on how to be inclusive of DIY AID, from discussing therapeutic options to supporting PWD during follow-up care, helping them improve their glycemic metrics and quality of life, and to lessen burden.
The nature of open-source insulin delivery systems is that the developers rapidly iterate adding new “branches” of code that allow for improvements in the system much faster than commercial AID systems, which require regulatory approval prior to making changes to algorithms and features. This may mean that, as soon as this user's guide is published, there could be new nuances to the system that will make it out of date. In reality, with the rapidly evolving evidence base in diabetes care today, this is true of all guidelines. The aim of this paper is to provide clinicians with an understanding of the evidence-based DIY AID systems reviewed in the corresponding position statement, which includes the following open-source systems: Loop, AndroidAPS, and OpenAPS. We recognize that additional open-source systems are available, such as iAPS (previously known as free APSX or FAX). While these systems have some similarities, there are additional settings and parameters that are beyond the scope of this paper. Additional adjustable parameters in newer branches of DIY algorithms may include terminology that does not build on existing continuous subcutaneous insulin infusion (CSII) language, making it difficult for HCPs to support individuals in optimizing settings; an effort by developers to consult with the diabetes education community would advance translation of DIY AID into clinical practice.
Discussing DIY AID as a Therapeutic Option
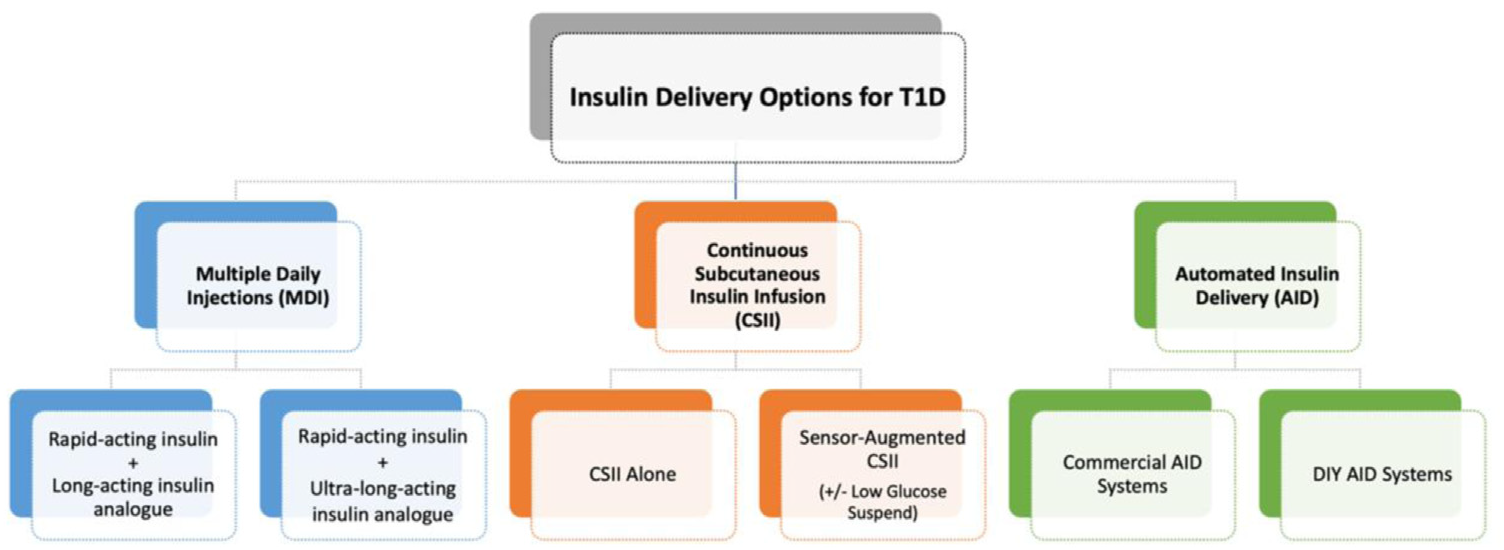
Clinicians may feel uncertain about if or how they should respond to or initiate discussions about DIY AID in practice. As highlighted in the position statement, HCPs should discuss all available treatment options that have evidence of benefit for PWD, together with risks and benefits. This encompasses varying levels of technology and AID, including both commercial and DIY options (Figure 1). We must challenge our own assumptions and biases which may influence the individuals with whom we discuss advanced technologies. Evidence has shown that some PWD whom HCPs may have assumed were not appropriate candidates for commercial AID were able to be successful and, in some cases, did better than those who were labelled as educated and technologically competent [1]. During treatment option discussions, it is imperative to use shared decision-making, while respecting autonomy, as PWD make choices about their best personal options. These options should be revisited on an ongoing basis given the dynamic nature of readiness for change, access to coverage, and alternative options available.
Figure 1
Including DIY AID as one of the insulin delivery options to discuss with people with T1D and their caregivers. DIY, do-it-yourself; T1D, type 1 diabetes.
Preparing PWD for a Successful Transition to DIY AID
While we encourage PWD to work through the steps of building their own DIY AID systems, we should provide guidance to help prepare them for a successful transition. Direct PWD to reliable resources for information, instructions, and support (Textbox 1
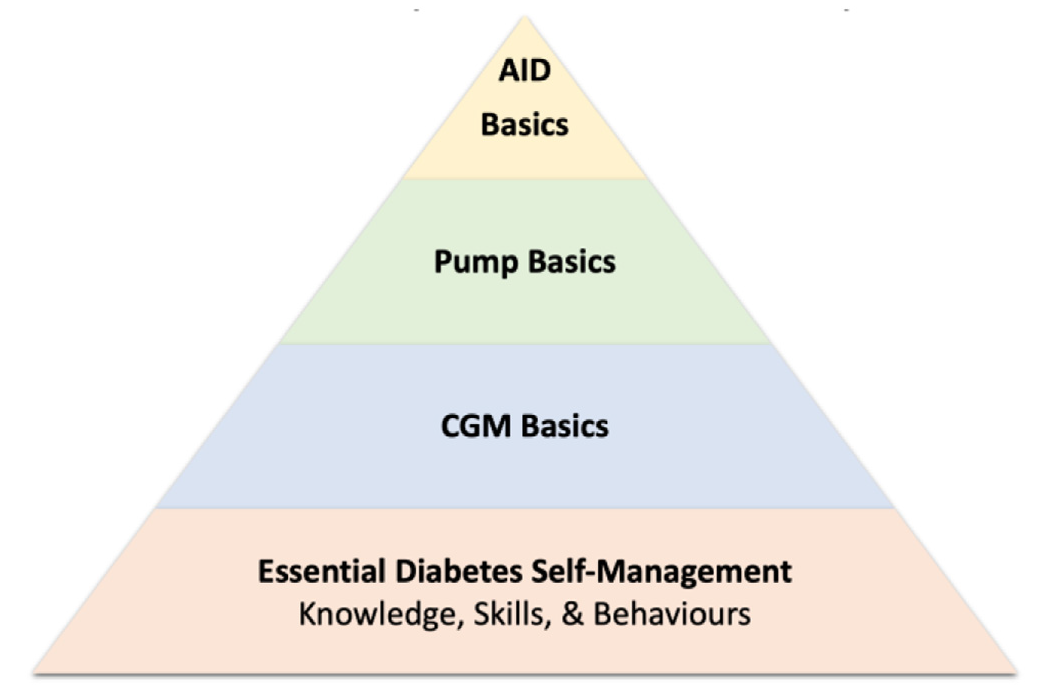
Clinically, preparation education should be comparable to CSII and commercial AID systems, including essential diabetes self-management education (e.g. troubleshooting hypo- and hyperglycemia, diabetic ketoacidosis prevention and treatment, etc.), the basic concepts of pump therapy and continuous glucose monitoring (CGM), and key concepts of AID (Figure 2
Textbox 1. DIY AID online resources
Community support:
Looped Facebook group (#WeAreNotWaiting): https://www.facebook.com/ groups/theloopedgroup/
Discord (#WeAreNotWaiting): https://discord.gg/hvugdvc5ms
Multiple other online message groups and forums have been reported to be sources of support for users of the various DIY AID systems, including Telegram, Zulipchapt, and Gitter.
System-specific information, education, and build instructions:
LoopDocs: https://loopkit.github.io/loopdocs/
OpenAPS’s documentation: https://openaps.readthedocs.io
Android APS’s documentation: https://androidaps.readthedocs.io
Education:
Automated Insulin Delivery (e-book): www.artificialpancreasbook.com
Loop and Learn: www.loopnlearn.org
Across all platforms, PWD are encouraged to start in “open-loop” first, where the system operates using the pump settings with no automation [3–5]. AndroidAPS users are forced to start in open-loop and are required to read and learn about all the features before the automation can be unlocked. HCPs can assist with evaluating pump settings before “closed-loop” functionality is initiated. While we encourage optimizing pump settings for safety and optimal performance, we emphasize that this does not translate to perfecting pump settings. The very nature of AID encompasses that automated delivery is able to compensate for inter- and intraday variability in insulin requirements, as well as accommodate for miscalculated (or sometimes even omitted) carbohydrate inputs. The focus should be on ensuring that the core pump settings are reflective of physiologic insulin requirements.
Finally, use shared decision-making to establish realistic and individualized goals. This should include not only numeric glycemic goals, but also personal goals about daily management and disease burden.
Figure 2
Essential education in preparation for do-it-yourself automated insulin delivery (AID) use. Prepared by Dr Revital Nimri and adapted from Phillip et al [2]. AID, automated insulin delivery; CGM, continuous glucose monitoring.
Navigating DIY AID to Optimize Settings
The high level of self-management taken on by PWD and/or their caregivers to use DIY AID systems is remarkable. While many will sacrifice considerable time and effort throughout initiation, HCPs should consider that the technological literacy skills for setup may differ from the health literacy skills required for evaluating settings and navigating diabetes management challenges [6]. While self-management in T1D is encouraged and support from the online community is very useful [7–9], HCP support remains invaluable.
The landscape of rapidly advancing diabetes technologies can be overwhelming. As with standard CSII and commercial AID systems, HCPs must have a basic understanding of the key system characteristics to effectively support PWD during follow-up care. This creates opportunities to collaborate on self-management plans and empower PWD as they strive to reach glycemic and personal goals, all while maintaining a trusting relationship with their HCPs.
Given the substantial differences across AID systems, the CARES paradigm was developed for HCPs to simplify understanding of the key characteristics for each system [10]. Applying the CARES framework to DIY AID systems allows us to address these clinically relevant questions (Figure 3
Calculate: How does the system calculate insulin delivery? [10]
Loop, AndroidAPS, and OpenAPS systems all use predictive algorithms, each with their own unique features [11]. The systems predict the future glucose by considering real-time CGM (rtCGM) data, current pump settings, active insulin, and recent carbohydrate inputs [3,4]. Insulin delivery is adjusted (up or down) to bring the predicted glucose into target range [3,4,6]. The programmed basal rates act as the baseline from which temporary basal adjustments and/or proportions of calculated boluses are made. Basal adjustments and automatic boluses are accounted for in active insulin/insulin on board (e.g. if basal rates are temporarily increased, the additional insulin is added to active insulin) [3]. Figure 4 shows how this information is displayed to the user.
Further details on the algorithms, including ongoing advancements to the systems, are openly available online (Textbox 1).
Adjust: How can the user adjust delivery? Which parameters can be user-adjusted? [10]
Understanding how to adjust insulin delivery is key for optimizing performance and safety. A key reason why many PWD choose DIY AID systems is the ability to customize more settings than with commercial systems [7,12]. DIY AID users have the ability to adjust nearly all standard pump settings (Textbox 2
New users are encouraged to evaluate and adjust pump settings prior to enabling “closed-loop” functionality to avoid inappropriate insulin delivery [3,6]; this includes those switching from multiple daily injections (MDI), standard CSII, or other AID systems. Pump settings should meet individual and physiological insulin requirements [6]. See Table 1
As with standard pump setting adjustments, users are encouraged to adjust 1 setting at a time to allow evaluation of the impact before proceeding further [4,5,10]. To evaluate settings, the combined CGM and insulin delivery data can be reviewed via Nightscout and/or Tidepool cloud-based systems (see Appendices A and B for report guides).
Some users choose to utilize the Autotune tool, which aids in calculating potential setting adjustments based on insulin delivery data. Careful consideration should be made to suggestions, and users are encouraged to review adjustments with their care teams. More information on Autotune is available at: https://openaps.readthedocs.io/en/latest/docs/customize-iterate/autotune.html.
Revert: When does the system revert to traditional pump settings (“open-loop”)? [10]
If CGM data and/or communication with the pump is disrupted, the system reverts from “closed-loop” to “open-loop” [10]. Insulin delivery will continue using the standard pump settings.
Users can manually revert to “open-loop” at any time. They should consider this during illness and/or ketosis, when potential prolonged suspensions may create risk [10], and during periods of inaccurate CGM performance. Users should follow CSII guidance on managing ketosis in the event of an infusion set/pod failure, including monitoring glucose levels and ketones, and administering manual corrective insulin. If a manual injection is required via insulin pen/syringe, closed-loop functionality should remain turned off for the duration of the insulin action time since insulin-on-board calculations will not be accurate [2]. To be prepared for unexpected periods of “open-loop,” we further emphasize the importance of assessing accuracy and safety of the standard pump settings and having a backup plan for subcutaneous injections should the pump or the infusion site fail.
Educate: What are the essential education points for safety and optimization of use? [10]
Users consistently report positive experiences with online support communities [6–9]; however, education from the health-care team remains important. Education should be individualized, empowering, and collaborative, supporting PWD in their self-management practices. Ongoing education should be comparable to other AID systems, including the key points outlined in Table 2
Textbox 2. Adjustable pump settings with DIY AID systems (Loop, AndroidAPS, OpenAPS)*
- Basal rates
- Insulin sensitivity factors
- Carbohydrate ratios
- Correction range (including a preprandial option)
- Insulin model (i.e. duration of insulin action or active insulin time)
- Delivery limits
- Suspend thresholds
* Additional parameters may require adjustments in newly developed DIY AID systems and may include terminology that does not build on existing continuous subcutaneous insulin infusion settings language.
In addition to the key education points in Table 2, HCPs and PWD should collaborate on individualized strategies for mealtime dosing, exercise/physical activity, and circumstances with varying insulin requirements (shift work, hormonal changes, steroid use, travel, etc.).
Mealtime dosing
Preprandial bolus delivery is important to optimize postprandial glycemia, and should be adjusted further if postprandial hyperglycemia persists despite validating pump settings. Users can adjust the time of the carbohydrate entry to indicate a prebolus or a delayed bolus (which results in a bolus recommendation that considers insulin adjustments already made). To help minimize excursions, users may explore using the preprandial correction range (Loop), which prompts the system to increase delivery in an attempt to reach this tighter target until the meal bolus is delivered. Advanced meal assist (OpenAPS) allows the system to set higher temporary basal increases more quickly following a meal bolus [11]. For challenges with high fat/protein meals, or responses to high and low glycemic index foods, the carbohydrate absorption time can be adjusted during the bolus entry, allowing the system to adjust accordingly. Users can track “carbohydrate on board” within their app (Figure 4). PWD should be reminded to follow mealtime bolus recommendations, unless adjusting for exercise or pending hypoglycemia; they should consider that bolus recommendations consider multiple factors, including previous insulin adjustments and future predictions. For safety, the system will not recommend a bolus if current or predicted glucose is below the suspend threshold. While users are encouraged to enter carbohydrate intake into the system [6], some PWD are able to utilize autocorrections and basal adjustments to cover individual varying amounts of carbohydrate. Some users may choose to log carbohydrate entries for hypoglycemia, but this is not required [3].
Physical activity and exercise
To maximize the potential for effectiveness, exercise management strategies with DIY AID should include adjusting the system target, minimizing peak insulin action during exercise, managing pre-exercise carbohydrate intake, and accounting for changes to insulin sensitivity (Table 3
Varying insulin requirements
In some situations, automated delivery adjustments may be sufficient to meet the needs of transient changes in insulin requirements, but this may not always be the case. In a recent qualitative study in women with T1D using DIY AID systems, most reported requiring additional adjustments according to their menstrual cycle [17]. In situations when automation alone is not sufficient, use of the temporary override should be discussed. Customized overrides can be saved to be used again as needed (see examples in Figure 5).
| Table 1 Clinical considerations for optimizing DIY AID settings |
|||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CGM, continuous glucose monitoring; DIY AID, do-it-yourself automated insulin delivery; IOB, insulin on board; ISF, insulin sensitivity factor; PWD, person with diabetes; T1D, type 1 diabetes; TDD, total daily dose. | |||||||||||||
| Step 1: Assess glycemia |
Assess if glycemic goals have been met, including time in target range, time below range, time above range, and glycemic variability (coefficient of variation). |
Step 2: Assess total daily dose |
Optimal TDD is an important factor for calculating and assessing physiological basal and bolus insulin pump settings [13]. If not meeting glycemic targets, consider an adjusted TDD for use with TDD-based insulin dose calculations (e.g. if time in hypoglycemic range is >4%, reduce TDD by 10%e20%; use the reduced TDD in basal and bolus setting calculations). When using a DIY AID system, the actual TDD may be more reflective of the optimal TDD, since the system adjusts insulin delivery regularly to minimize hypo- and hyperglycemia [13]. |
Step 3: Evaluate basal rates |
Prioritize basal rate evaluation, as inaccuracies may impair the accuracy of bolus settings [3,6,13].
Actual basal delivery may be much higher than the total of programmed basal rates if the algorithm uses basal adjustments for corrections and/or covering unannounced carbohydrate intake. Consider this when assessing % basal. Practice tip: When assessing and adjusting basal rates, compare the actual basal delivery with the programmed basal rates. Look for what happens in the absence of food and activity: ➔ Consistently increasing basal (resulting in positive IOB): basal rates may be too low. Confirm if this is related to missed carbohydrate boluses. ➔ Consistently decreasing basal (resulting in negative IOB), especially if glucose drops below range: basal rates may be too high [3]. |
Step 4: Evaluate bolus settings |
Insulin sensitivity factor (ISF): ➔ If ISF is too strong: correction boluses and basal adjustments will be more aggressive when the glucose is predicted to be above target, and may result in hypoglycemia. ➔ If ISF is too weak, correction boluses and basal adjustments will be insufficient to achieve glucose targets. Practice tip: Watch for fluctuating glucose levels among new DIY AID users, which are commonly linked with an inaccurate ISF [3]. For example, an ISF that is too strong will lead the system to overcompensate for both predicted high and low glucose levels, leading to a “roller coaster”—like glucose curve in the absence of food. Carbohydrate ratios (CRs): |
Additional setting considerations: Insulin model |
The recommended models for all current rapid-acting insulins (including faster-acting aspart) default to 6-hour insulin action time [3], which reflects the pharmacodynamic profiles. Encourage using the 6-hour models to minimize insulin stacking [3,6].
Practice tip: If switching from other systems, consider how using different models may impact other settings (i.e. switching from a 3-hour to a 6-hour duration time may require strengthening the ISF). |
Correction range |
The correction range (or single value) is the glucose level that the system corrects to. Preprandial override target: |
Safety settings |
With DIY AID, users can customize settings beyond the abilities of commercial systems, where many delivery limits are set by the manufacturers. Therefore, extra attention should be drawn to these settings for safety: Maximum basal rate:
Maximum bolus:
Suspend threshold:
CGM alerts: |
| Table 2 Key self-management education points for DIY AID users (adapted from [10]) |
|
|---|---|
| Note: Core diabetes self-management, CGM, and CSII education remains essential with the use of DIY AID. CGM, continuous glucose monitoring; CR, carbohydrate ratio; CSII, continuous subcutaneous insulin infusion; DIY AID, do-it-yourself automated insulin delivery; PWD, person with diabetes; T1D, type 1 diabetes. | |
| 1. Establish and individualize goals and expectations |
Collaborate to set realistic goals, while avoiding over-reliance on numeric targets [6]. Address personal goals around daily management and burden [6]. |
| 2. Adjust insulin pump settings to optimize performance |
Review how to assess and self-adjust settings to reflect physiological requirements. Watch for inaccurate settings that may compensate for one another (e.g. a strong ISF that is compensating for an inaccurately weak CR and resulting in excess hypoglycemia). |
| 3. Trust the system (minimize bolus overrides) |
Over-interaction with the system may increase glycemic variability [1]. Discuss how insulin on board accumulates from temp basal increases and/or automatic boluses; overriding bolus recommendations may result in hypoglycemia. |
| 4. Pre-bolus for meals |
Initiate bolus delivery before eating (typically 10e20 minutes) to optimize postprandial glucose levels [2]. Adjust timing by considering meal composition, pre-meal glucose level, presence of gastroparesis, and individual patterns. ➔ 30e60 minutes: consider decreasing by 50% ➔ >60 minutes: deliver system-recommended correction boluses only, as needed |
| 5. Consider altering hypoglycemia treatment |
Less carbohydrate may be required, depending on duration of suspension prior to a hypoglycemic event [6,10]. |
| 6. Use “Override Presets” or “Temporary Targets” to meet temporarily changing needs (e.g. increased/decreased activity levels, hormonal fluctuations, steroid use, travel) |
This allows users to temporarily adjust the target range and/or insulin settings (basal rates, CRs, and ISFs) by a uniform percentage over a selected duration [3,6]. |
| 7. Review best practices for site management |
Discuss site selection and rotation, skin preparation, and adhesion tips for both infusion sets/pods and sensors. |
| 8. Review backup plan |
Review considerations for reverting to open-loop or standard pump therapy (i.e. consider use of temp basal rates; may need to weaken CRs). |
| 9. Know where to find reliable support and resources |
Ensure PWD are familiar with the #WeAreNotWaiting online support group and open access documents for detailed information on their system (Textbox 1). |
| Table 3 Exercise adjustment factors to consider with DIY AID systems [2,6] |
||||
|---|---|---|---|---|
| Note: Adapt these suggestions based on individual glycemic responses to various forms of exercise (see examples in Figure 5). Competitive and elite athletes will likely require further customized strategies. | ||||
| Exercise type | Glucose target | Carbohydrate management | Insulin delivery settings | Postexercise management |
| Aerobic exercise(e.g. walking, running, cycling, etc) | 1e2 hours before exercise: set a higher glucose target | Within 3 hours of exercise: reduce carbohydrate bolus by 25%–75% 15–60 minutes before exercise: if possible/ desirable, avoid carbohydrate intake to minimize insulin on board (unless needed for pending hypoglycemia). Immediately before, at onset, and/or during exercise: consume small amounts of simple carbohydrate as needed (without entering into system) | >1 hour before exercise: adjust temporary insulin delivery profiles to deliver ~50% less basal and bolus insulin. Use the “Override Preset” (Loop) or adjust the “Sensitivity Ratio” (OpenAPS and AndroidAPS) to allow insulin delivery to be adjusted accordingly, including basal and bolus settings. | At completion or up to 6 hours postexercise: Cancel temporary target and changes to insulin delivery settings. Maintain adjustments up to 6 hours, if needed, to minimize postexercise hypoglycemia. Postexercise boluses may require reduction up to 50%. Monitor glucose levels and adapt insulin delivery as needed. |
| Anaerobic exercise(e.g. weightlifting, sprints, strength training, etc) | Glucose targets may not require adjustment. | May not require insulin adjustments. Monitor individual patterns. | Up to 3–4 hours postexercise: consider tightening glucose targets and temporarily increasing insulin delivery profile, if needed, to avoid hyperglycemia. Consider risk of nocturnal hypoglycemia. | |
| Table 4 Approach to accessing data for review during a clinical encounter |
||
|---|---|---|
| CGM, continuous glucose monitoring. | ||
| Steps | Nightscout tab | Tidepool tab |
| 1. Insulin delivery settings | Profiles | Device settings (not currently available with Loop) |
| 2. CGM metrics | Distribution | Basics or trends |
| 3. Ambulatory glucose profile "Graphical View" | Percentile chart | Trends |
| 4. Daily graph of CGM and insulin delivery | Day to day | Daily |
Sensor/share: What are the relevant characteristics of the compatible CGM sensor(s) and sharing capabilities? [10]
The list of compatible rtCGM devices continues to evolve as sensor technology advances. Users should follow recommendations from the CGM manufacturer on calibration and confirmation CBG requirements, as applicable. Sharing capabilities are available for CGM systems via manufacturer apps. HCPs may recommend that PWD using DIY AID systems connect to Nightscout or Tidepool. These open-source cloud-based platforms provide glucose and insulin delivery metrics and daily graphs, which include CGM tracings, along with basal rate modulations, carbohydrates entered, and bolus delivered. A step-by-step approach to looking at Tidepool and Nightscout reports can be found in Table 4
Figure 3
The CARES framework: Highlighting the key points of automated insulin delivery systems [10].

Figure 4
Sample home screen displays from do-it-yourself automated insulin delivery systems demonstrating real-time calculations. CGM, continuous glucose monitoring.

Figure 5
Customized use of the temporary override feature by Loop users. Both cases above illustrate use of multiple customized temporary override settings, including individual targets, for various activity levels. (A) Case 1 uses a 50% reduction of her overall insulin needs as a starting point to feel comfortable with most exercise. She has reduced this further for more intense activity (“Very Active” setting). She is setting up a Ski Day profile with a 30% reduction since she has learned from her patterns that she does not need to reduce as much for skiing as other activities. (B) Case 2 is an experienced Loop user who enjoys being very active. Over time, she has refined her override settings to allow her the flexibility to fit activity into her life, even after a meal, while maintaining glucose levels in her personal target range. She is able to effectively minimize her risks for hypoglycemia during exercise.

Future Developments
When new system updates become available, it is imperative that users prioritize learning about new features. AndroidAPS systems require users to complete training modules with each system update. For other systems, users should read the updated documentation on their system-specific resource site (Textbox 1).
As new versions of AID DIY systems are developed, HCPs are encouraged to continue applying the CARES paradigm to facilitate ongoing understanding and to allow for continued support for PWD who choose to use these systems.
Frequently Asked Questions
How is safety maintained when people are downloading “code” from the internet without regulatory approval?
The developers of these systems are themselves living with T1D or they are caregivers of someone with T1D. Safety and avoidance of hypoglycemia is the primary objective. The open-source documents detail that users build the systems at their own risk and that all updates to the system will be tested with volunteers. PWD should stay engaged with the community to ensure they are aware of any suggested safety updates and are encouraged to upgrade their software to include the newer updates to the algorithm.
If a PWD has an adverse event (severe hypoglycemia, diabetic ketoacidosis) while using these systems, can I be found negligent/liable if I have supported them?
People with T1D have no choice but to manage their condition with life-sustaining insulin therapy that comes with an inherent risk of severe complications. It is the responsibility of the HCP to educate PWD and ensure they have the skills necessary to avoid these complications by monitoring and adjusting their insulin, glucose levels, and ketones, when necessary, regardless of the method of insulin delivery (commercial AID, basal/bolus therapy, insulin pump therapy with/without CGM, etc). To our knowledge, DIY AID has never been tested in the Canadian courts, so we can only provide the advice that all methods of insulin delivery carry the same risks, and HCP support and education are critical to ensuring safe outcomes.
Can I refuse to support PWD using a technology I am not comfortable with?
If an HCP is confronted with something outside their scope, they have an obligation to inform the individual it is not in their scope of practice and to refer on. That being said, HCPs who care for people with diabetes should make themselves familiar with all treatments available for both T1D and T2D to the best of their ability. It may not be realistic for HCPs who have low volumes of T1D in their practice to become experts in AID, and referral to someone with more expertise can and should be considered within the confines of provincial resources. It should be expected that if an HCP provides support for individuals with T1D who use commercial AID systems, they should provide similar support to a person who chooses DIY AID.
Is there a risk of using an out of warranty pump to deliver insulin?
All technology has a risk of failure. When a pump is in warranty, the company has an obligation to replace it; after the warranty has expired, this obligation is no longer enforceable under law, though many pump manufacturers will provide a loaner pump for some duration of time to bridge the individual until new funding is available. In some provinces and territories, the warranty duration is shorter than funding cycles for new pumps, meaning many PWD will be using an out-of-warranty pump regardless of the AID system they choose to use. All PWD should have a backup plan with an understanding of how to transition back to open-loop if a CGM fails or MDI if the pump fails, again, regardless of the AID system they choose.
How can I view the insulin and glucose sensor data from the PWD in my practice who are on DIY AID?
Nightscout is an open-source solution developed by PWD that provides browser-based visualization for DIY AID users. It allows retrospective analysis and remote monitoring which help facilitate HCP interactions.
Tidepool is a free platform that allows DIY loop users to upload their glucose, carbohydrate, and insulin delivery data to their account and share their data with their clinician.
What happens if the PWD does not have their phone or goes “offline”?
The algorithm uses Bluetooth technology to communicate between the CGM, the phone, and the pump, so, as long as the phone is on, the PWD does not need access to the internet for AID to continue. If the phone dies or is left at home, the PWD will continue to receive insulin based on their programmed basal rates. They should monitor glucose levels more closely since the system will not adjust delivery to prevent hypo- or hyperglycemia.
What if CGM readings are inaccurate for a time period; how will this impact insulin delivery?
Similar to those using commercial AID, PWD should be encouraged to perform a fingerstick glucose reading any time their symptoms do not match their sensor readings. CGM low and high alerts should be used, including snooze/repeat times, to prompt PWD to take action and problem solve when sensor glucose is reading in the hypo- and hyperglycemic ranges. Delivery settings should be set appropriately (Table 1) to minimize the potential for excessive over or under delivery of insulin. If the sensor is not reading accurately, closed-loop functionality should be temporarily turned off until the sensor has been replaced. Some PWD choose to use third-party adaptors that convert intermittently scanned CGM into rtCGM to enable AID; there is an added level of uncertainty with accuracy and reliability in these cases and PWD should be encouraged to fingerstick regularly.
Supplementary Material
To access the supplementary material accompanying this article, visit the online version of the Canadian Journal of Diabetes at www.canadianjournalofdiabetes.com.
Author Disclosures
I.J.H. has received speaker and advisory board fees from Dexcom Canada, Abbott Diabetes Canada and Sanofi unrelated to the current work; H.O.W is funded by a Canada Research Chair in Human-Centred Digital Health, has lived with type 1 diabetes since 1983, and has used a DIY AID since 2019; A.C. has received speaker fees from Dexcom Canada, Abbott Diabetes Canada, consulting fees from Dexcom Canada, and insulin pump training fees from Insulet, Medtronic and Tandem, she lives with type 1 diabetes and has personal experience using both DIY AID and commercially available AID systems (Medtronic and Tandem); P.S. is supported by the Charles A. Allard Chair in Diabetes Research and the Alberta Academic Medicine and Health Services Plan and has received personal fees for consulting for Vertex, Novo Nordisk and Viatris; K.F. is a member of the Nightscout Foundation board of directors; A.E.M. has no conflicts.
Appendix A: Tidepool Key Report Guide (for Loop)
Tidepool use tips [3]:
- Users will need to install the Tidepool Mobile app on their phone, create an account, and follow the steps on LoopDocs (below). CGM, insulin delivery, carbohydrate data, and notes will sync without the need for an uploader.
- To view Tidepool reports on a computer, the Chrome web browser must be used.
- If data is not visible at first, ensure the user has entered a note in their Tidepool Mobile app.
- Loop settings are not visible in the Device Settings report, since this information cannot be uploaded from Apple Health. To obtain device settings, ask users to show you or capture screenshots of their device settings directly from their Loop app.
For additional information on using Tidepool with Loop, including options to set up a clinic account, visit: https://loopkit.github.io/looptips/data/tidepool.
Figure A1
Sharing data with a clinic.

Figure A2
Tidepool trends report. A1C, glycated hemoglobin; BG, blood glucose; CGM, continuous glucose monitoring; TDD, total daily dose. * Recommended targets from the International Consensus Report for most individuals with type 1 diabetes. Individualize glycemic goals based on individual goals and circumstances, and for special populations (pregnancy, children/adolescents, older/high-risk groups).

Figure A3
Tidepool daily report.

Appendix B: Nightscout Key Report Guide
Nightscout use tips:
- Users will need to create a Nightscout account and follow the set-up instructions in the documentation for their specific system (Table 1).
- Nightscout allows for real-time remote monitoring and review of multiple reports.
- Users can share their individual web address to share their data.
- To view reports from the real-time data home screen, click on the drop-down main menu (top right), and choose REPORTS.
More information on Nightscout is available at: https://nightscout.github.io.
Figure B1
Navigating the Nightscout report settings.

Figure B2
Nightscout distribution report.

Figure B3
Nightscout percentile chart report.

Figure B4
Nightscout day-to-day report.

Figure B5
Nightscout profiles report.

References
- Lawton J, et al. Health professionals' views about who would benefit from using a closed-loop system: A qualitative study. Diabet Med 2020;37:1030-1037.
- Phillip M, Nimri R, Bergenstal RM, et al. Consensus recommendations for the use of automated insulin delivery technologies in clinical practice. Endocr Rev 2023;44:254-280.
- Loopdocs. https://loopkit.github.io/loopdocs. Accessed August 22, 2022.
- OpenAPS. https://openaps.readthedocs.io/en/latest. Accessed September 29, 2022.
- Android APS. https://androidaps.readthedocs.io/en/latest. Accessed September 29, 2022.
- Braune K, et al. Open-source automated insulin delivery: International consensus statement and practical guidance for health-care professionals. Lancet Diabetes Endocrinol 2022;10:58-74.
- Suttiratana SC, et al. Qualitative study of user experiences with loop, an open-source automated insulin delivery system. Diabetes Technol Ther 2022;24:416-423.
- Braune K, Krug N, Knoll C, Ballhausen H, Thieffry A, Chen Y, et al. Emotional and physical health impact in children and adolescents and their caregivers using open-source automated insulin delivery: Qualitative analysis of lived experiences. J Med Internet Res 2022;4:e37120.
- Van Os M, PW, De Galan B, Bazelmans E, Tack C, Metz A, Nefs G. Healthcare needs of adults with type 1 diabetes considering, in transfer to or using do-it-yourself closed loop systems, in ATTD. 2022.
- Messer LH, Berget C, Forlenza GP. A clinical guide to advanced diabetes devices and closed-loop systems using the CARES paradigm. Diabetes Technol Ther 2019;21:462-469.
- Lal RA, et al. Realizing a closed-loop (artificial pancreas) system for the treatment of type 1 diabetes. Endocr Rev 2019;40:1521-1546.
- Walsh J, et al. Insulin titration guidelines for patients with type 1 diabetes: It is about time! J Diabetes Sci Technol 2022. 19322968221087261.
- Walsh J, et al. Insulin titration guidelines for patients with type 1 diabetes: It is about time! J Diabetes Sci Technol 2022. 19322968221087261.
- Chan AJ, Halperin IJ. Beyond glycated hemoglobin: Harnessing data from sensor-based technology to improve glucose variability, time in range and hypoglycemia in adult patients with type 1 diabetes. Can J Diabetes 2021;45:269-72. e3.
- Cemeroglu AP, et al. Basal and bolus insulin requirements in children, adolescents, and young adults with type 1 diabetes mellitus on continuous subcutaneous insulin infusion (CSII): Effects of age and puberty. Endocr Pract 2013;19:805-811.
- Riddell MC, et al. Exercise management in type 1 diabetes: A consensus statement. Lancet Diabetes Endocrinol 2017;5:377-390.
- Mewes D, et al. Variability of glycemic outcomes and insulin requirements throughout the menstrual cycle: A qualitative study on women with type 1 diabetes using an open-source automated insulin delivery system. J Diabetes Sci Technol 2022. 19322968221080199.
Diabetes Canada is the registered owner of all content on guidelines.diabetes.ca and ShopDC. For questions, please email info@diabetes.ca